

Multi-layered repair of high-flow CSF fistulae following endoscopic skull base surgery without nasal packing or lumbar drains: technical refinements to optimise outcome
- PMID: 37074392
- PMCID: PMC10409672
- DOI: 10.1007/s00701-023-05581-y
Multi-layered repair of high-flow CSF fistulae following endoscopic skull base surgery without nasal packing or lumbar drains: technical refinements to optimise outcome
Abstract
Aims: Post-operative CSF leak remains a significant problem following endoscopic skull base surgery, particularly when there is a high-flow intra-operative CSF leak. Most skull base repair techniques are accompanied by the insertion of a lumbar drain and/or the use of nasal packing which have significant shortcomings. Our aim was to review the results of a large series of endoscopic skull base cases where a high-flow intra-operative CSF leak rate was encountered and repaired to assess if modifications in technique could reduce the post-operative CSF leak rate.
Methods: A retrospective review of a prospectively maintained database of skull base cases performed by a single surgeon over a 10-year period was performed. Data regarding patient demographics, underlying pathology, skull base repair techniques and post-operative complications were analysed.
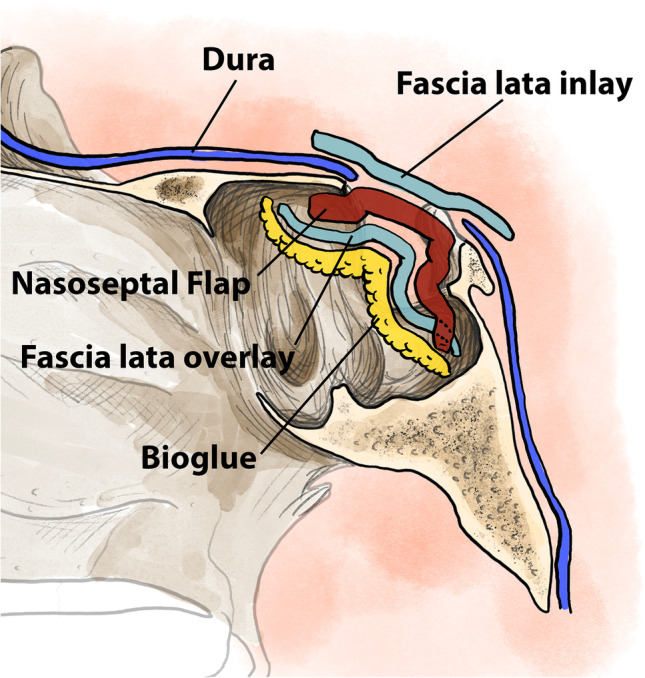
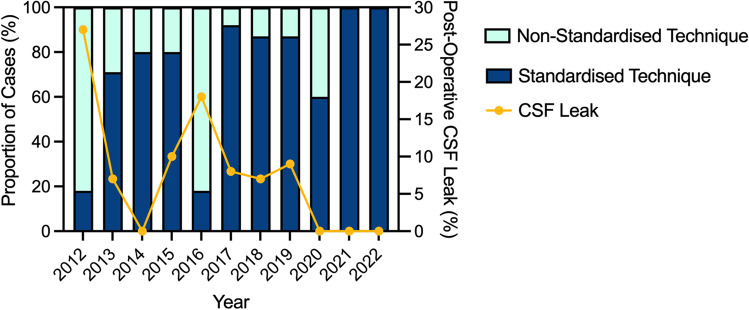
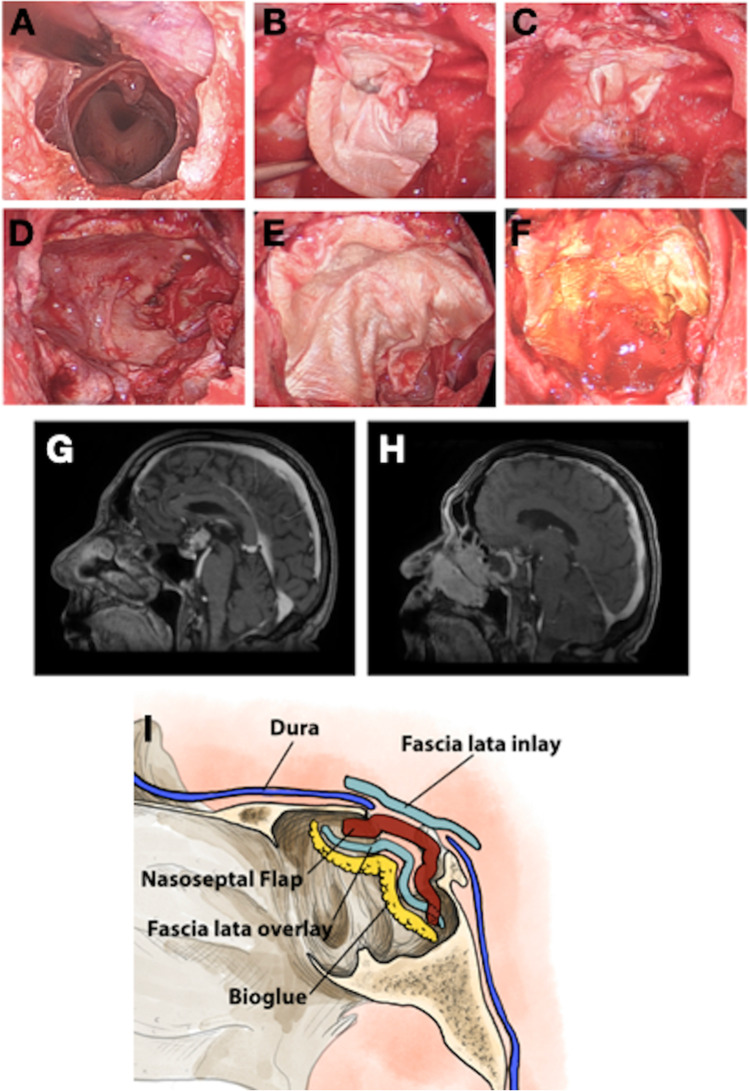
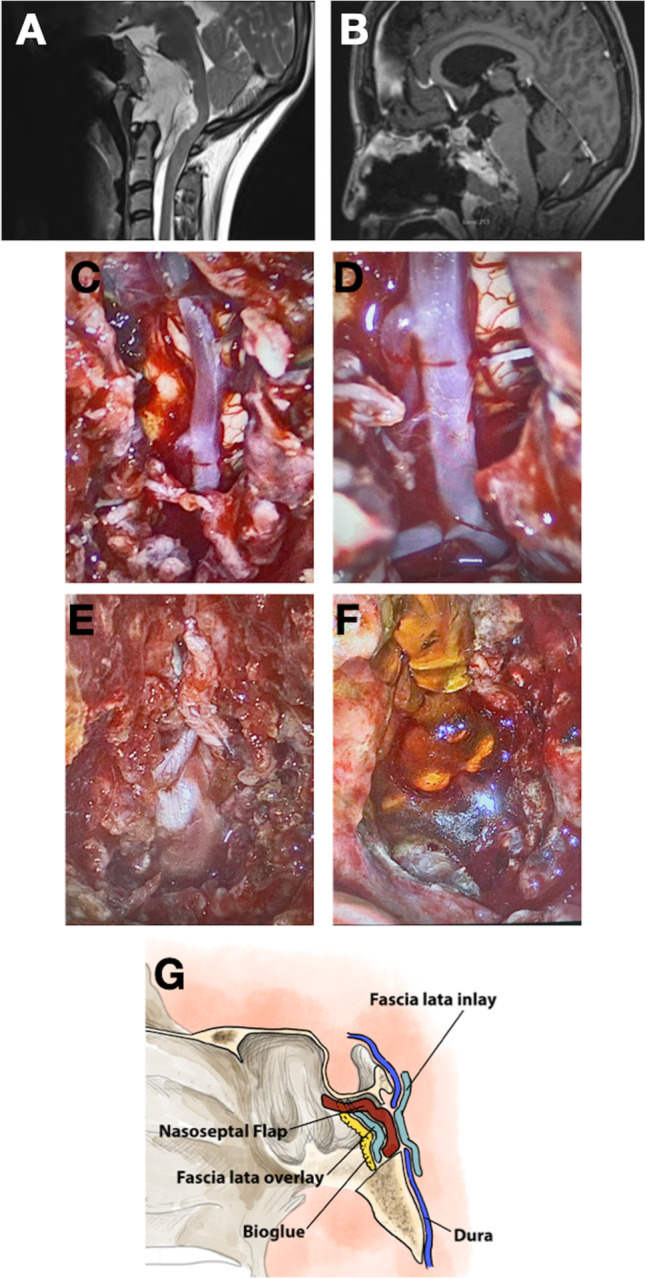
Results: One hundred forty-two cases with high-flow intra-operative CSF leak were included in the study. The most common pathologies were craniopharyngiomas (55/142, 39%), pituitary adenomas (34/142, 24%) and meningiomas (24/142, 17%). The CSF leak rate was 7/36 (19%) when a non-standardised skull base repair technique was used. However, with the adoption of a standardised, multi-layer repair technique, the post-operative CSF leak rate decreased significantly (4/106, 4% vs. 7/36, 19%, p = 0.006). This improvement in the rate of post-operative CSF leak was achieved without nasal packing or lumbar drains.
Conclusion: With iterative modifications to a multi-layered closure technique for high-flow intra-operative CSF leaks, it is possible to obtain a very low rate of post-operative CSF leak, without lumbar drains or nasal packing.
Keywords: CSF leak; Chordoma; Endoscopic skull base; Meningioma; Pituitary adenoma; Skull base.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Conger A, Zhao F, Wang X, Eisenberg A, Griffiths C, Esposito F, Carrau RL, Barkhoudarian G, Kelly DF. Evolution of the graded repair of CSF leaks and skull base defects in endonasal endoscopic tumor surgery: trends in repair failure and meningitis rates in 509 patients. J Neurosurg. 2018;130:861–875. doi: 10.3171/2017.11.Jns172141. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
