

Association between prehospital end-tidal carbon dioxide levels and mortality in patients with suspected severe traumatic brain injury
- PMID: 37074395
- PMCID: PMC10205841
- DOI: 10.1007/s00134-023-07012-z
Association between prehospital end-tidal carbon dioxide levels and mortality in patients with suspected severe traumatic brain injury
Abstract
Purpose: Severe traumatic brain injury is a leading cause of mortality and morbidity, and these patients are frequently intubated in the prehospital setting. Cerebral perfusion and intracranial pressure are influenced by the arterial partial pressure of CO2 and derangements might induce further brain damage. We investigated which lower and upper limits of prehospital end-tidal CO2 levels are associated with increased mortality in patients with severe traumatic brain injury.
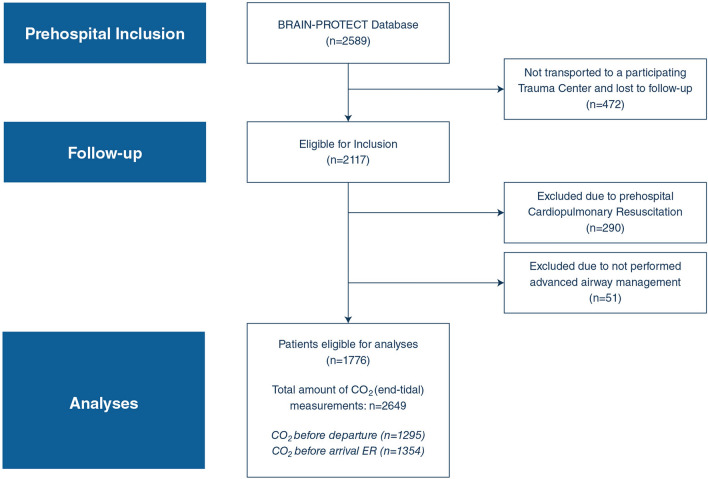
Methods: The BRAIN-PROTECT study is an observational multicenter study. Patients with severe traumatic brain injury, treated by Dutch Helicopter Emergency Medical Services between February 2012 and December 2017, were included. Follow-up continued for 1 year after inclusion. End-tidal CO2 levels were measured during prehospital care and their association with 30-day mortality was analyzed with multivariable logistic regression.
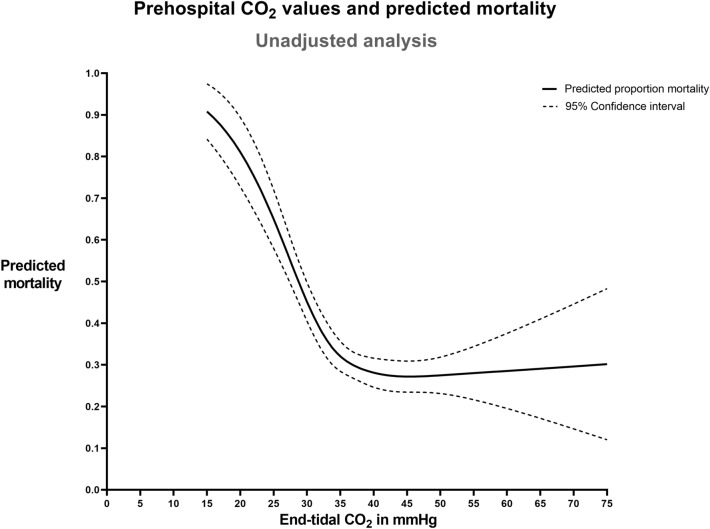
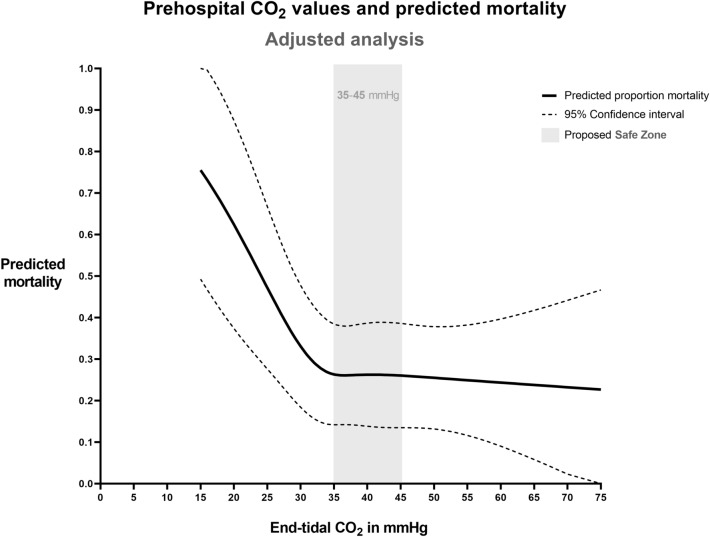
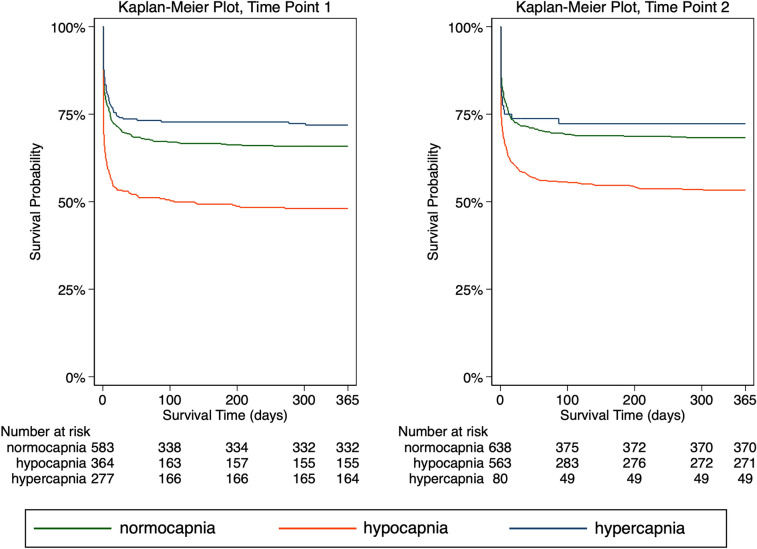
Results: A total of 1776 patients were eligible for analysis. An L-shaped association between end-tidal CO2 levels and 30-day mortality was observed (p = 0.01), with a sharp increase in mortality with values below 35 mmHg. End-tidal CO2 values between 35 and 45 mmHg were associated with better survival rates compared to < 35 mmHg. No association between hypercapnia and mortality was observed. The odds ratio for the association between hypocapnia (< 35 mmHg) and mortality was 1.89 (95% CI 1.53-2.34, p < 0.001) and for hypercapnia (≥ 45 mmHg) 0.83 (0.62-1.11, p = 0.212).
Conclusion: A safe zone of 35-45 mmHg for end-tidal CO2 guidance seems reasonable during prehospital care. Particularly, end-tidal partial pressures of less than 35 mmHg were associated with a significantly increased mortality.
Keywords: Carbon dioxide; Critical care; Endotracheal intubation; Traumatic brain injury; Ventilation.
© 2023. The Author(s).
Conflict of interest statement
SMB reported receiving grants from Achmea Healthcare Foundation during the conduct of the study. ARA reported receiving grants and personal fees from Becton Dickson and The Medicines Company; grants from Draeger; sponsor-initiated and funded phase 1 research from Rigel; and personal fees from PAION, Janssen Pharma, Ever Pharma, and Philips outside the submitted work. PS reported receiving grants from Dutch Brain Foundation and Achmea Healthcare Foundation during the conduct of the study. No other disclosures were reported.
Figures
Comment in
-
Prehospital ventilation targets in severe traumatic brain injury.Intensive Care Med. 2023 May;49(5):554-555. doi: 10.1007/s00134-023-07044-5. Epub 2023 Apr 15. Intensive Care Med. 2023. PMID: 37060441 No abstract available.
References
-
- Bossers SM, Boer C, Bloemers FW, Van Lieshout EMM, Den Hartog D, Hoogerwerf N, Innemee G, van der Naalt J, Absalom AR, Peerdeman SM, de Visser M, de Leeuw MA, Schwarte LA, Loer SA, Schober P, (2020) Epidemiology, Prehospital Characteristics and Outcomes of Severe Traumatic Brain Injury in The Netherlands: The BRAIN-PROTECT Study. Prehospital emergency care: official journal of the National Association of EMS Physicians and the National Association of State EMS Directors: 1–12
-
- Gravesteijn BY, Sewalt CA, Stocchetti N, Citerio G, Ercole A, Lingsma HF, von Steinbüchel N, Steyerberg EW, Wilson L, Maas AIR, Menon DK, Lecky FE. Prehospital Management of Traumatic Brain Injury across Europe: A CENTER-TBI Study. Prehospital Emerg Care. 2021;25:629–643. doi: 10.1080/10903127.2020.1817210. - DOI - PubMed
-
- Badjatia N, Carney N, Crocco TJ, Fallat ME, Hennes HM, Jagoda AS, Jernigan S, Letarte PB, Lerner EB, Moriarty TM, Pons PT, Sasser S, Scalea T, Schleien CL, Wright DW, (2008) Guidelines for prehospital management of traumatic brain injury 2nd edition. Prehospital emergency care : official journal of the National Association of EMS Physicians and the National Association of State EMS Directors 12 Suppl 1: S1–52 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
