

Etiology, Presentation, and Risk Factors for Diarrheal Syndromes in 3 Sub-Saharan African Countries After the Introduction of Rotavirus Vaccines From the Vaccine Impact on Diarrhea in Africa (VIDA) Study
- PMID: 37074436
- PMCID: PMC10116565
- DOI: 10.1093/cid/ciad022
Etiology, Presentation, and Risk Factors for Diarrheal Syndromes in 3 Sub-Saharan African Countries After the Introduction of Rotavirus Vaccines From the Vaccine Impact on Diarrhea in Africa (VIDA) Study
Abstract
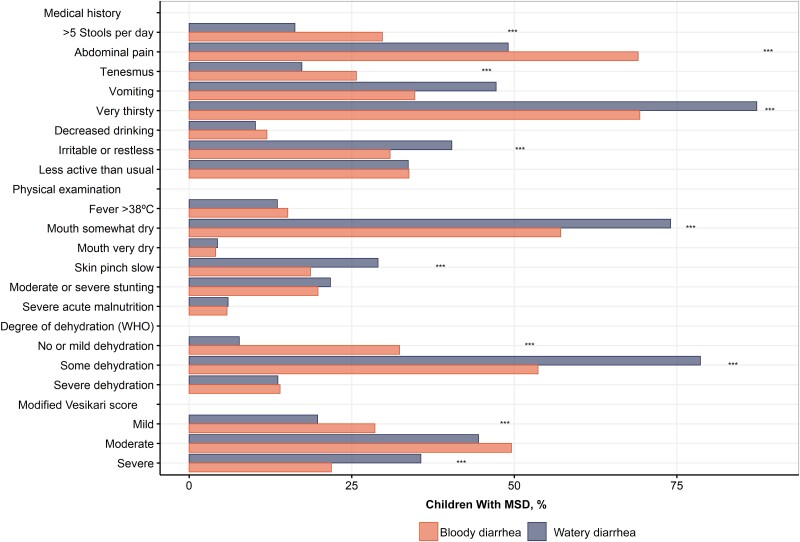
Background: Diarrheal disease is heterogeneous, including watery diarrhea (WD) and dysentery, some cases of which become persistent diarrhea (PD). Changes in risk over time necessitate updated knowledge of these syndromes in sub-Saharan Africa.
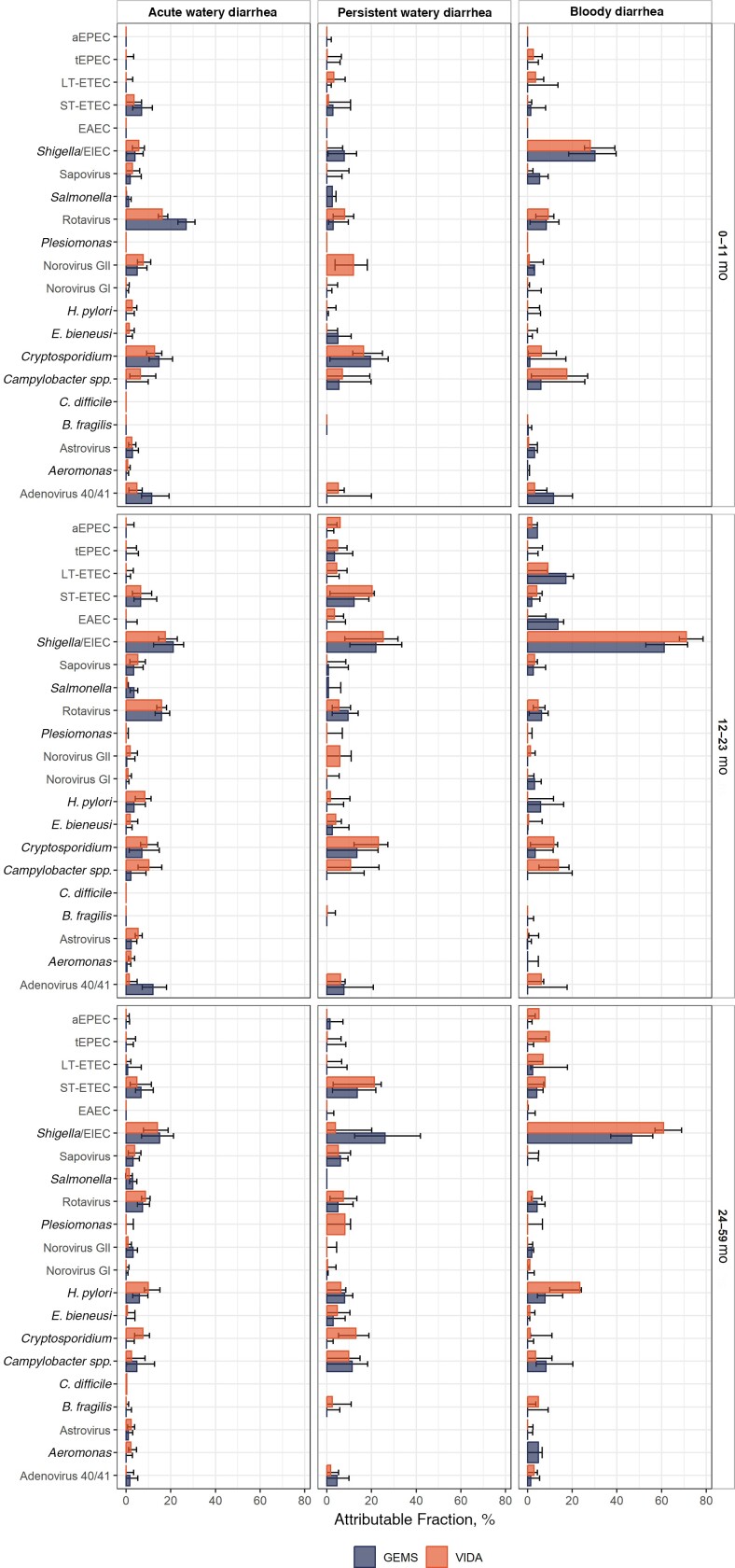
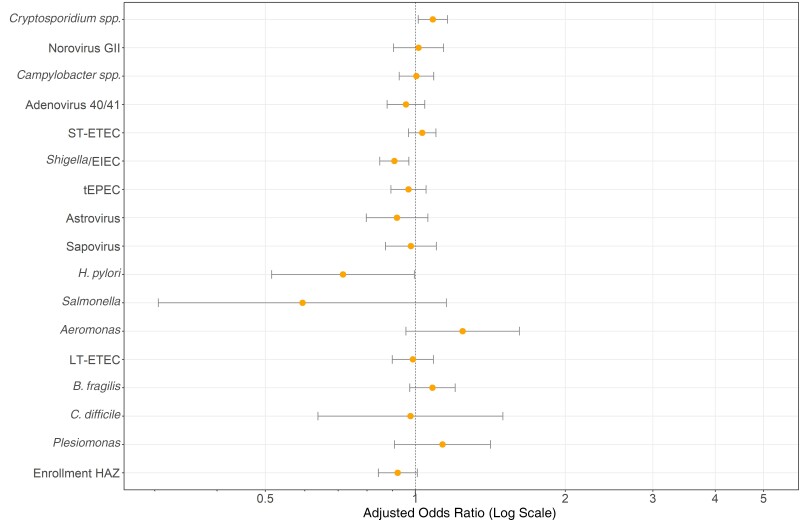
Methods: The Vaccine Impact on Diarrhea in Africa (VIDA) study was an age-stratified, case-control study of moderate-to-severe diarrhea among children <5 years old in The Gambia, Mali, and Kenya (2015-2018). We analyzed cases with follow-up of about 60 days after enrollment to detect PD (lasting ≥14 days), examined the features of WD and dysentery, and examined determinants for progression to and sequelae from PD. Data were compared with those from the Global Enteric Multicenter Study (GEMS) to detect temporal changes. Etiology was assessed from stool samples using pathogen attributable fractions (AFs), and predictors were assessed using χ2 tests or multivariate regression, where appropriate.
Results: Among 4606 children with moderate-to-severe diarrhea, 3895 (84.6%) had WD and 711 (15.4%) had dysentery. PD was more frequent among infants (11.3%) than in children 12-23 months (9.9%) or 24-59 months (7.3%), P = .001 and higher in Kenya (15.5%) than in The Gambia (9.3%) or Mali (4.3%), P < .001; the frequencies were similar among children with WD (9.7%) and those with dysentery (9.4%). Compared to children not treated with antibiotics, those who received antibiotics had a lower frequency of PD overall (7.4% vs 10.1%, P = .01), and particularly among those with WD (6.3% vs 10.0%; P = .01) but not among children with dysentery (8.5% vs 11.0%; P = .27). For those with watery PD, Cryptosporidium and norovirus had the highest AFs among infants (0.16 and 0.12, respectively), while Shigella had the highest AF (0.25) in older children. The odds of PD decreased significantly over time in Mali and Kenya while increasing significantly in The Gambia.
Conclusions: The burden of PD endures in sub-Saharan Africa, with nearly 10% of episodes of WD and dysentery becoming persistent.
Keywords: diarrhea; dysentery; global; infection; persistent.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. S. M. T. reports multiple grants paid to her institution from the National Institutes of Health, the Bill & Melinda Gates Foundation, Wellcome Trust, Affinivax, Lumen Biosciences, PATH, and the Medical Research Council. S. M. T. also reports payments as royalties related to intellectual property for Salmonella vaccines and Klebsiella/Pseudomonas vaccines; consulting fees and travel support from the University of Washington for a grant proposal; multiple planned, issued, and pending patents on Salmonella, Klebsiella, and Pseudomonas vaccines; and multiple unpaid committee roles with the American Society of Tropical Medicine and Hygiene. K. L. K. reports consultation fees and travel support from PATH and the University of Washington related to diarrheal diseases and grant support to her institution from the National Institute of Allergy and Infections Diseases, Institut Pasteur, and the Bill & Melinda Gates Foundation. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Briend A, Aziz K, Hasan KZ, Hoque B. Are diarrhoea control programmes likely to reduce childhood malnutrition? Observations from rural Bangladesh. Lancet 1989; 334:319–22. - PubMed
-
- Kuşkonmaz B, Yurdakök K, Yalcin S, Ozmert E. Comparison of acute bloody and watery diarrhea: a case control study. Turk J Pediatr 2009; 51:133–40. - PubMed
-
- Ronsmans C, Bennish M, Wierzba T. Diagnosis and management of dysentery by community health workers. Lancet 1988; 332:552–5. - PubMed
