

Clinical and Epidemiologic Features of Cryptosporidium-Associated Diarrheal Disease Among Young Children Living in Sub-Saharan Africa: The Vaccine Impact on Diarrhea in Africa (VIDA) Study
- PMID: 37074443
- PMCID: PMC10116562
- DOI: 10.1093/cid/ciad044
Clinical and Epidemiologic Features of Cryptosporidium-Associated Diarrheal Disease Among Young Children Living in Sub-Saharan Africa: The Vaccine Impact on Diarrhea in Africa (VIDA) Study
Abstract
Background: As part of the Vaccine Impact on Diarrhea in Africa (VIDA) Study, we examined the prevalence, clinical presentation, and seasonality of Cryptosporidium in children to understand its relative burden after the introduction of rotavirus vaccine.
Methods: VIDA was a 3-year, age-stratified, matched case-control study of medically attended acute moderate-to-severe diarrhea (MSD) in children aged 0-59 months residing in censused populations at sites in Kenya, Mali, and The Gambia. Clinical and epidemiologic data were collected at enrollment, and a stool sample was tested for enteropathogens by quantitative PCR. An algorithm was created based on the organism's cycle threshold (Ct) and association with MSD to identify the subset of Cryptosporidium PCR-positive (Ct <35) cases most likely to be attributed to MSD. Clinical outcomes were assessed at 2-3 months after enrollment.
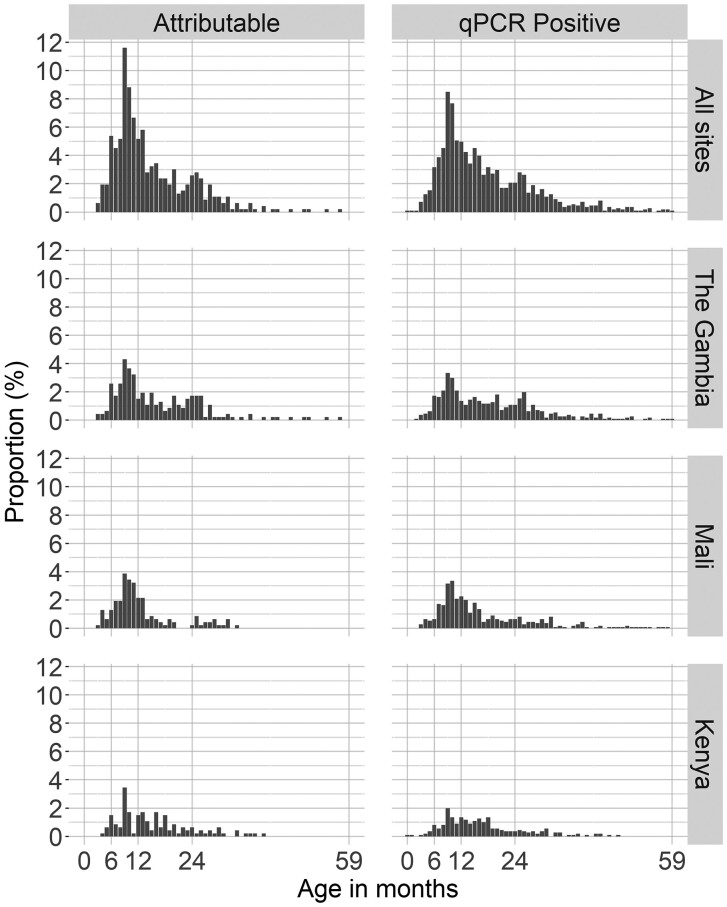
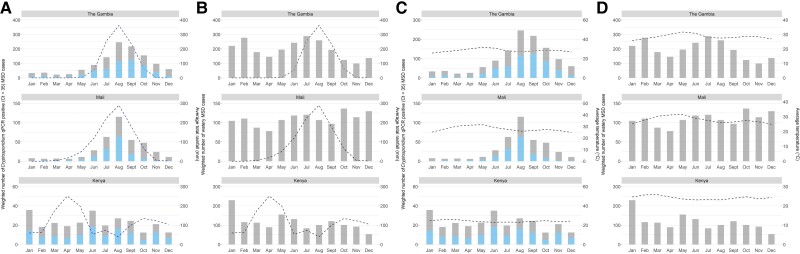
Results: One thousand one hundred six (22.9%) cases of MSD and 873 controls (18.1%) were PCR positive for Cryptosporidium; 465 cases (42.0%) were considered attributable to Cryptosporidium, mostly among children 6-23 months. Cryptosporidium infections peaked in The Gambia and Mali during the rainy season, while in Kenya they did not have clear seasonality. Compared with cases with watery MSD who had a negative PCR for Cryptosporidium, cases with watery MSD attributed to Cryptosporidium were less frequently dehydrated but appeared more severely ill using a modified Vesikari scale (38.1% vs 27.0%; P < 0.001), likely due to higher rates of hospitalization and intravenous fluid administration, higher prevalence of being wasted or very thin very thin (23.4% vs 14.7%; P < 0.001), and having severe acute malnutrition (midupper arm circumference <115 mm, 7.7% vs 2.5%; P < 0.001). On follow-up, Cryptosporidium-attributed cases had more prolonged and persistent episodes (43.2% vs 32.7%; P <0 .001) and linear growth faltering (change in height-for-age z score between enrollment and follow-up: -0.29 vs -0.17; P < 0.001).
Conclusions: The burden of Cryptosporidium remains high among young children in sub-Saharan Africa. Its propensity to cause illness and further impact children longer term by compromising nutritional status early in life calls for special attention to enable appropriate management of clinical and nutritional consequences.
Keywords: Cryptosporidium; children; diarrhea; prevalence; severity.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . E. R. H. reports financial support from the Bill and Melinda Gates Foundation (OPP1129479). K. L. K. reports consultation fees and travel support from PATH and the University of Washington related to diarrheal diseases and grant support to her institution from the National Institutes of Health, Institut Pasteur, and the Bill & Melinda Gates Foundation. S. M. T. reports multiple grants paid to her institution from the National Institutes of Health (NIH), Bill & Melinda Gates Foundation (BMGF), Wellcome Trust, Affinivax, Lumen Biosciences, PATH, and Medical Research Council. She also reports payments as royalties related to intellectual property for Salmonella vaccines and Klebsiella/Pseudomonas vaccines and consulting fees and travel support from the University of Washington for a grant proposal. She also reports holding multiple planned, issued, and pending patents on Salmonella, Klebsiella, and Pseudomonas vaccines and hold multiple unpaid committee roles with the American Society of Tropical Medicine and Hygiene. S. R. C. H. reports salary funding from the UK Medical Research Council and the University of Auckland. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Kotloff KL, Nataro JP, Blackwelder WC, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): a prospective, case-control study. Lancet 2013; 382:209–22. - PubMed
-
- Molbak K, Andersen M, Aaby P, et al. Cryptosporidium infection in infancy as a cause of malnutrition: a community study from Guinea-Bissau, West Africa. Am J Clin Nutr 1997; 65:149–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
