

Place in Therapy of Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: A Targeted Literature Review
- PMID: 37074594
- PMCID: PMC10191980
- DOI: 10.1007/s11523-023-00957-7
Place in Therapy of Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: A Targeted Literature Review
Abstract
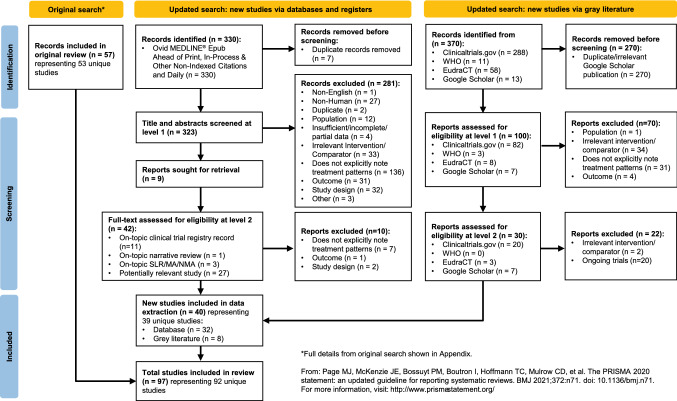
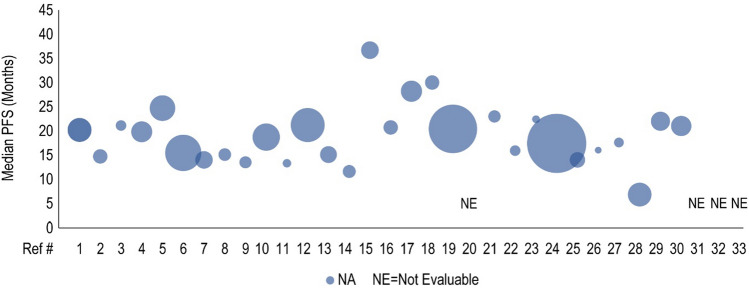
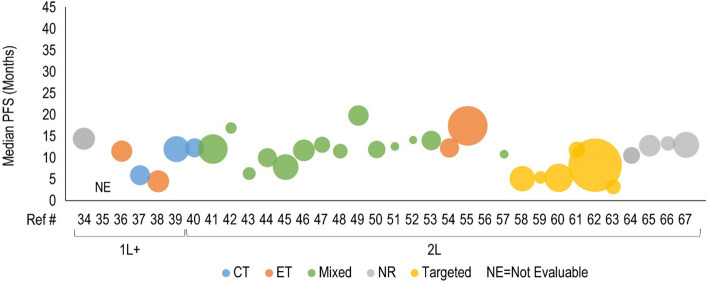
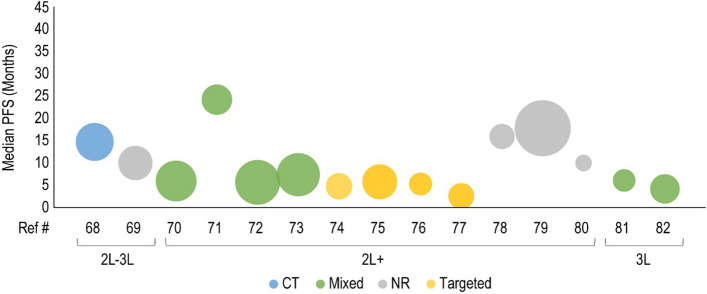
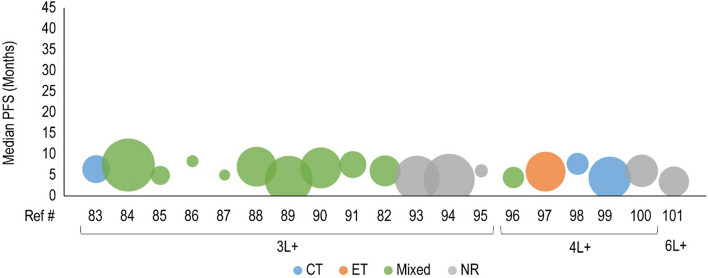
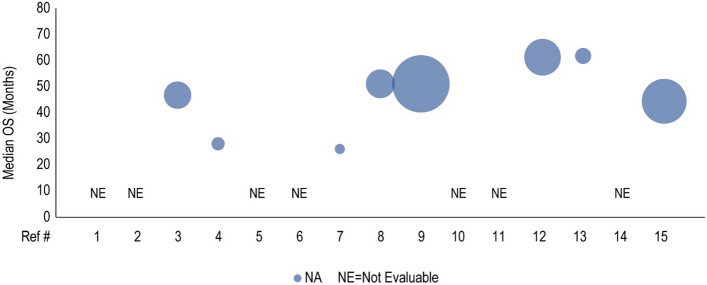
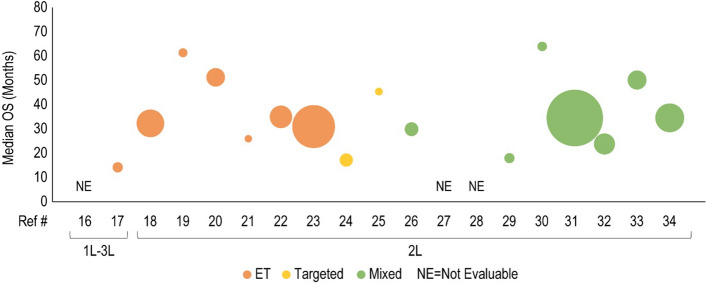
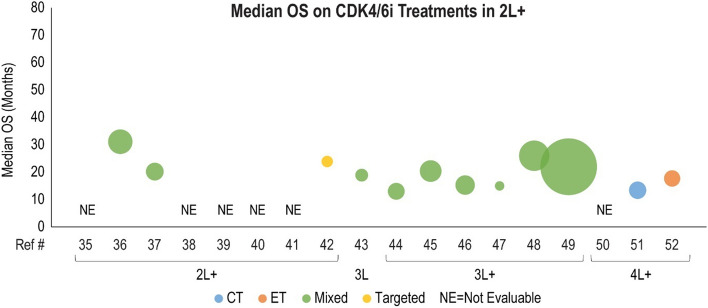
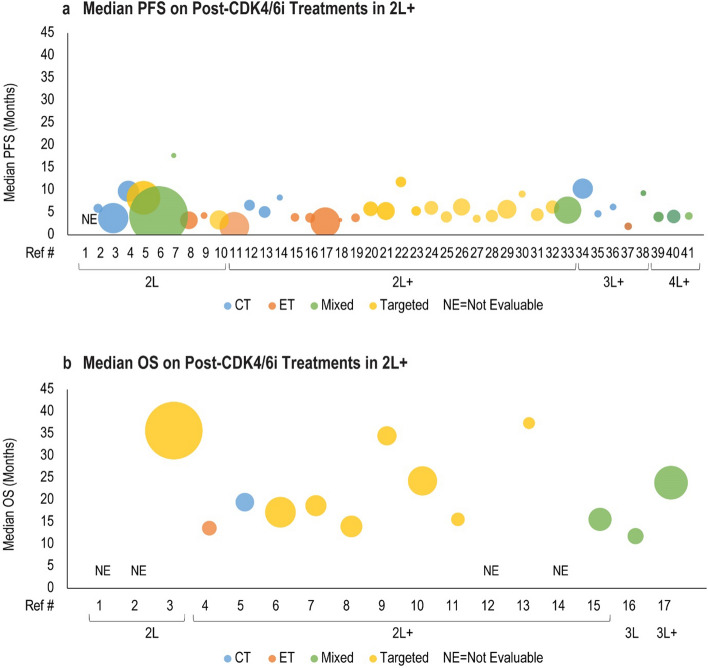
Cyclin-dependent kinase 4 and 6 inhibitors (CDK4/6i) are the preferred regimen for patients with hormone receptor-positive and human epidermal growth factor receptor 2-negative (HR+/HER2-) advanced or metastatic breast cancer. However, the optimal treatment sequencing for CDK4/6i with other available therapeutic options is unclear. We conducted a targeted literature review to identify the current evidence on CDK4/6i treatment patterns in patients with breast cancer. The search was initially conducted in October 2021 and subsequently updated in October 2022. Biomedical databases and gray literature were searched, and bibliographies of included reviews were screened for relevant studies. The search identified ten reviews published since 2021 and 87 clinical trials or observational studies published since 2015. The included reviews discussed CDK4/6i usage with or without endocrine therapy (ET) in first-line and second-line treatment for patients with HR+/HER2- advanced or metastatic breast cancer, followed by ET, chemotherapy, or targeted therapy with ET. Clinical studies reported similar treatment sequences consisting of ET, chemotherapy, or targeted therapy with ET prior to CDK4/6i with ET, followed by ET monotherapy, chemotherapy, targeted therapy with ET, or continued CDK4/6i with ET. Current evidence suggests CDK4/6i are effective for HR+/HER2- advanced or metastatic breast cancer in earlier lines of therapy. Efficacy of CDK4/6i as measured by progression-free survival and overall survival was similar within a line of therapy regardless of the type of prior therapy. Survival on different post-CDK4/6i treatments was also similar within the same line of therapy. Additional research is needed to investigate the optimal place in therapy of CDK4/6i and the sequencing of treatments following progression on CDK4/6i.
© 2023. The Author(s).
Conflict of interest statement
Melody Zhao, Yixie Zhang, and Anna Zhou are employees of EVERSANA, which was a paid consultant to Pfizer in connection with the development of this manuscript. Kent A. Hanson is an employee of University of Illinois at Chicago, which was a paid consultant to Pfizer in connection with the development of this manuscript. Ashley S. Cha-Silva is an employee of and stockholder in Pfizer Inc. Alexis Jenkins, Rhett Figliuzzi, Amanda Griffin, Michaela Spence, and Manvir Rai are employees of EVERSANA. Becky Skidmore is a contractor of EVERSANA.
Figures
References
-
- NIH SEER Program. Cancer stat facts: female breast cancer subtypes. 2022. https://seer.cancer.gov/statfacts/html/breast-subtypes.html. Accessed 21 Mar 2023.
-
- Blows FM, Driver KE, Schmidt MK, Broeks A, Van Leeuwen FE, Wesseling J, et al. Subtyping of breast cancer by immunohistochemistry to investigate a relationship between subtype and short and long term survival: a collaborative analysis of data for 10,159 cases from 12 studies. PLoS Med. 2010;7(5):e1000279. doi: 10.1371/journal.pmed.1000279. - DOI - PMC - PubMed
-
- Breastcancer.org. Breast cancer stages. 2022. https://www.breastcancer.org/pathology-report/breast-cancer-stages. Accessed 21 Mar 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
