

The association between antihypertensive treatment and serious adverse events by age and frailty: A cohort study
- PMID: 37075078
- PMCID: PMC10155987
- DOI: 10.1371/journal.pmed.1004223
The association between antihypertensive treatment and serious adverse events by age and frailty: A cohort study
Abstract
Background: Antihypertensives are effective at reducing the risk of cardiovascular disease, but limited data exist quantifying their association with serious adverse events, particularly in older people with frailty. This study aimed to examine this association using nationally representative electronic health record data.
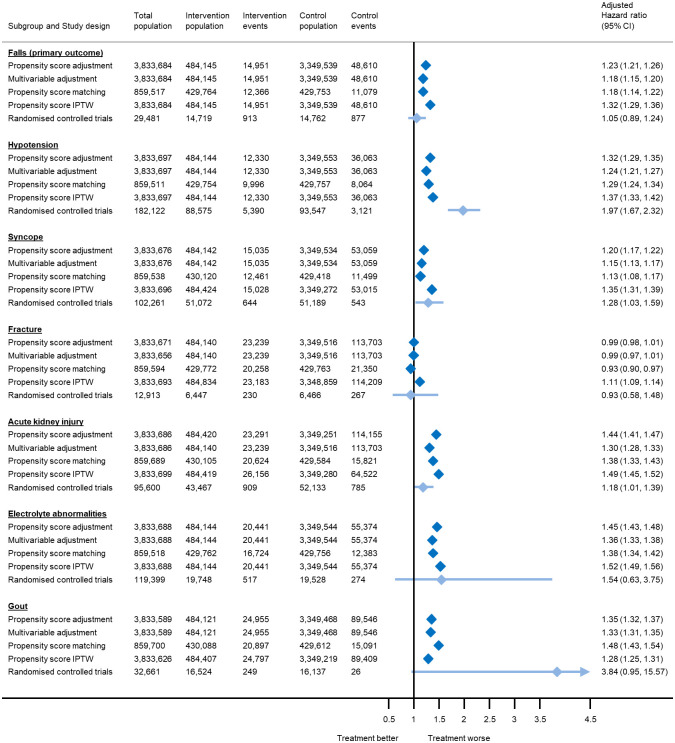
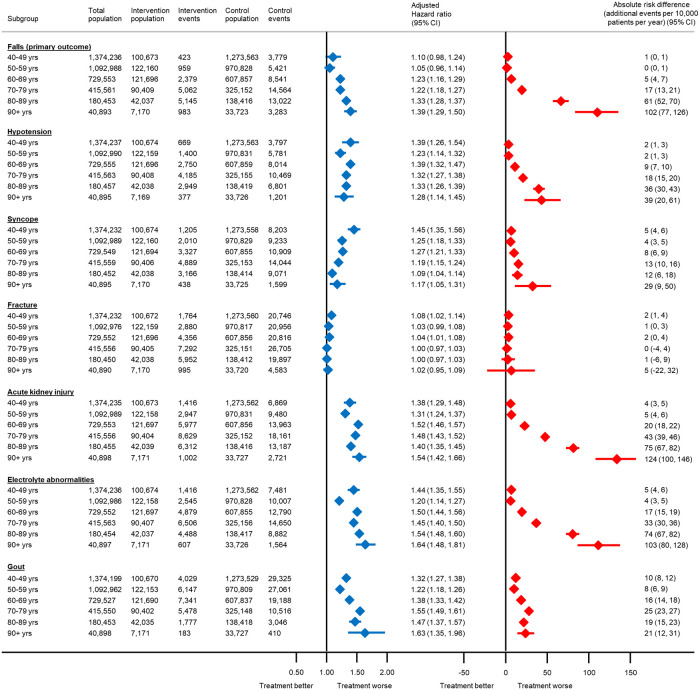
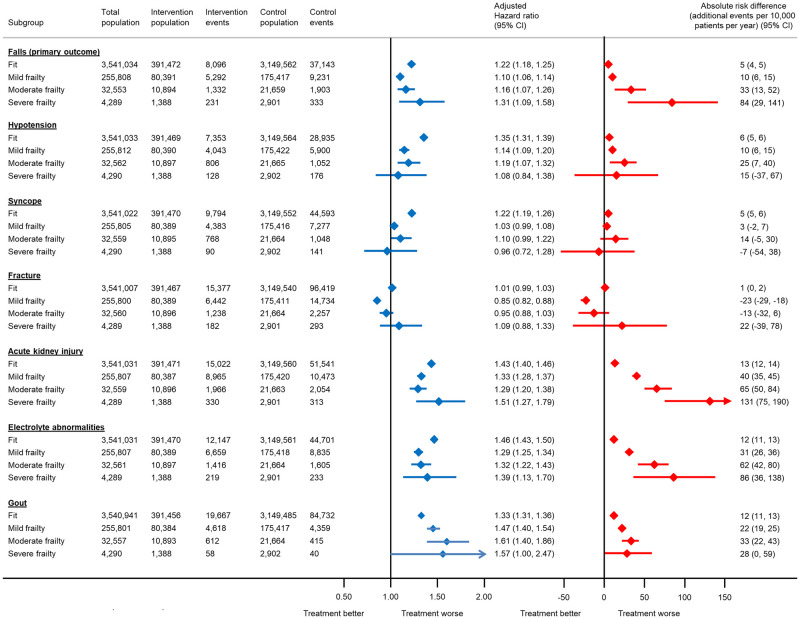
Methods and findings: This was a retrospective cohort study utilising linked data from 1,256 general practices across England held within the Clinical Practice Research Datalink between 1998 and 2018. Included patients were aged 40+ years, with a systolic blood pressure reading between 130 and 179 mm Hg, and not previously prescribed antihypertensive treatment. The main exposure was defined as a first prescription of antihypertensive treatment. The primary outcome was hospitalisation or death within 10 years from falls. Secondary outcomes were hypotension, syncope, fractures, acute kidney injury, electrolyte abnormalities, and primary care attendance with gout. The association between treatment and these serious adverse events was examined by Cox regression adjusted for propensity score. This propensity score was generated from a multivariable logistic regression model with patient characteristics, medical history and medication prescriptions as covariates, and new antihypertensive treatment as the outcome. Subgroup analyses were undertaken by age and frailty. Of 3,834,056 patients followed for a median of 7.1 years, 484,187 (12.6%) were prescribed new antihypertensive treatment in the 12 months before the index date (baseline). Antihypertensives were associated with an increased risk of hospitalisation or death from falls (adjusted hazard ratio [aHR] 1.23, 95% confidence interval (CI) 1.21 to 1.26), hypotension (aHR 1.32, 95% CI 1.29 to 1.35), syncope (aHR 1.20, 95% CI 1.17 to 1.22), acute kidney injury (aHR 1.44, 95% CI 1.41 to 1.47), electrolyte abnormalities (aHR 1.45, 95% CI 1.43 to 1.48), and primary care attendance with gout (aHR 1.35, 95% CI 1.32 to 1.37). The absolute risk of serious adverse events with treatment was very low, with 6 fall events per 10,000 patients treated per year. In older patients (80 to 89 years) and those with severe frailty, this absolute risk was increased, with 61 and 84 fall events per 10,000 patients treated per year (respectively). Findings were consistent in sensitivity analyses using different approaches to address confounding and taking into account the competing risk of death. A strength of this analysis is that it provides evidence regarding the association between antihypertensive treatment and serious adverse events, in a population of patients more representative than those enrolled in previous randomised controlled trials. Although treatment effect estimates fell within the 95% CIs of those from such trials, these analyses were observational in nature and so bias from unmeasured confounding cannot be ruled out.
Conclusions: Antihypertensive treatment was associated with serious adverse events. Overall, the absolute risk of this harm was low, with the exception of older patients and those with moderate to severe frailty, where the risks were similar to the likelihood of benefit from treatment. In these populations, physicians may want to consider alternative approaches to management of blood pressure and refrain from prescribing new treatment.
Copyright: © 2023 Sheppard et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al.. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension (Dallas, Tex: 1979). 2018;71(6):e13–e115. Epub 2017/11/15. doi: 10.1161/HYP.0000000000000065 . - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
