

Regional spreading pattern is associated with clinical phenotype in amyotrophic lateral sclerosis
- PMID: 37075222
- PMCID: PMC10545526
- DOI: 10.1093/brain/awad129
Regional spreading pattern is associated with clinical phenotype in amyotrophic lateral sclerosis
Abstract
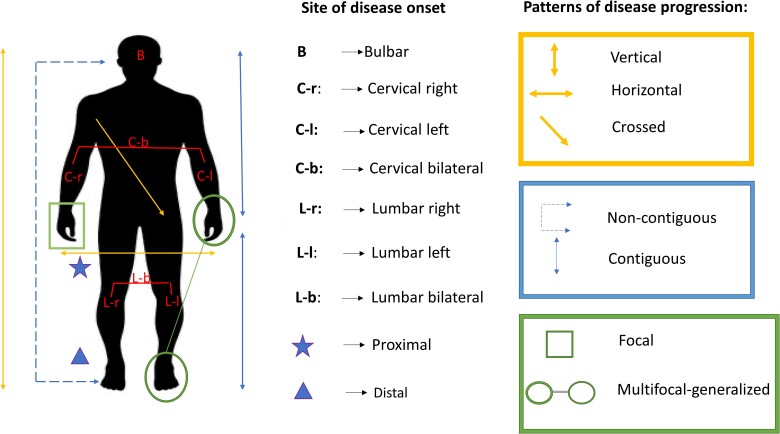
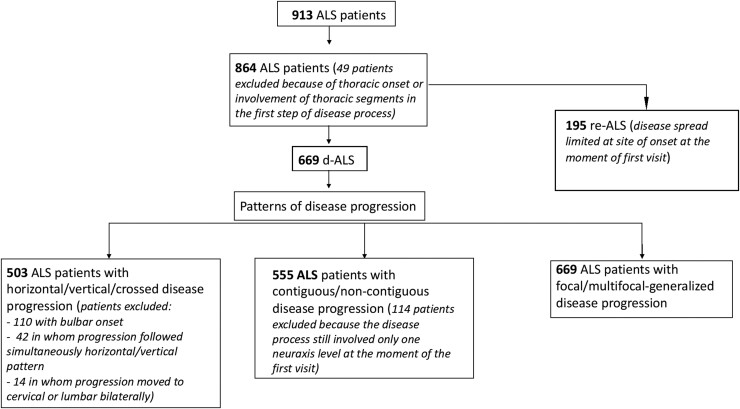
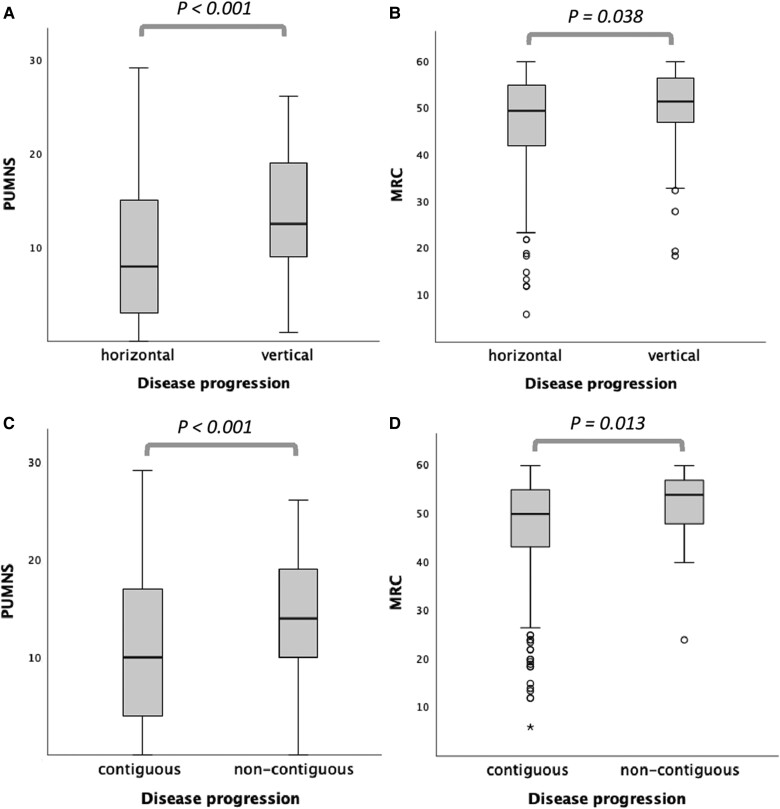
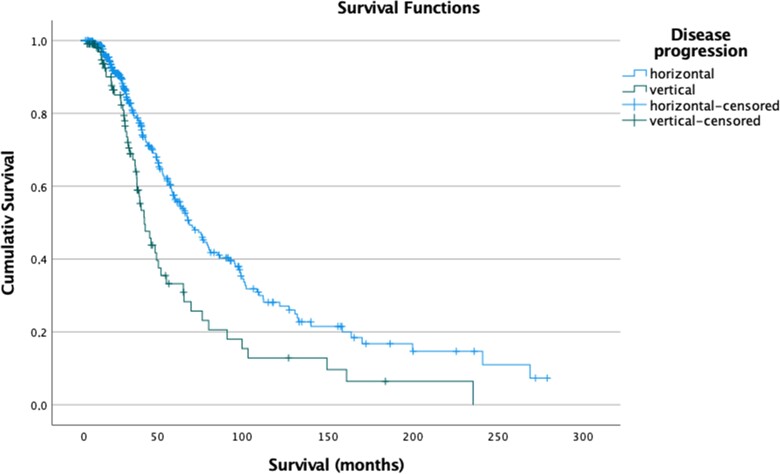
Increasing evidence shows that disease spreading in amyotrophic lateral sclerosis (ALS) follows a preferential pattern with more frequent involvement of contiguous regions from the site of symptom onset. The aim of our study was to assess if: (i) the burden of upper (UMN) and lower motor neuron (LMN) involvement influences directionality of disease spreading; (ii) specific patterns of disease progression are associated with motor and neuropsychological features of different ALS subtypes (classic, bulbar, primary lateral sclerosis, UMN-predominant, progressive muscular atrophy, flail arm, flail leg); and (iii) specific clinical features may help identify ALS subtypes, which remain localized to the site of onset for a prolonged time (regionally entrenching ALS). A single-centre, retrospective cohort of 913 Italian ALS patients was evaluated to assess correlations between directionality of the disease process after symptom onset and motor/neuropsychological phenotype. All patients underwent an extensive evaluation including the following clinical scales: Penn Upper Motor Neuron Score (PUMNS), MRC Scale for Muscle Strength and the Edinburgh Cognitive and Behavioural ALS Screen (ECAS). The most frequent initial spreading pattern was that towards adjacent horizontal regions (77.3%), which occurred preferentially in patients with lower MRC scores (P = 0.038), while vertical diffusion (21.1%) was associated with higher PUMNS (P < 0.001) and with reduced survival (P < 0.001). Non-contiguous disease spreading was associated with more severe UMN impairment (P = 0.003), while contiguous disease pattern with lower MRC scores. Furthermore, non-contiguous disease spreading was associated with more severe cognitive impairment in both executive and visuospatial ECAS domains. Individuals with regionally entrenching ALS were more frequently female (45.6% versus 36.9%; P = 0.028) and had higher frequencies of symmetric disease onset (40.3% versus 19.7%; P < 0.001) and bulbar phenotype (38.5% versus 16.4%; P < 0.001). Our study suggests that motor phenotypes characterized by a predominant UMN involvement are associated with a vertical pattern of disease progression reflecting ipsilateral spreading within the motor cortex, while those with predominant LMN involvement display more frequently a horizontal spreading from one side of the spinal cord to the other. These observations raise the hypothesis that one of the mechanisms underlying disease spreading in ALS pathology is represented by diffusion of toxic factors in the neuron microenvironment. Finally, it is possible that in our cohort, regionally entrenching ALS forms are mainly observed in patients with atypical bulbar phenotypes, characterized by a slowly progressive course and relatively benign prognosis.
Keywords: amyotrophic lateral sclerosis (ALS); disease progression; motor neuron disease (MND); motor phenotype; site of onset; somatotopic organization of motor system.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
A.M., F.V., E.C., B.P., A.D., R.B., D.G. M.M., L.M., S.M., S.C. and C.M. report no disclosure. V.S. received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, LiquidWeb Srl and Novartis Pharma AG. He receives or has received research support from the Italian Ministry of Health, AriSLA, and E-Rare Joint Translational Call. He is on the Editorial Board of
Figures
References
-
- van Es MA, Hardiman O, Chio A, et al. Amyotrophic lateral sclerosis. Lancet. 2017;390:2084–2098. - PubMed
-
- Burrell JR, Halliday GM, Kril JJ, et al. The frontotemporal dementia-motor neuron disease continuum. Lancet. 2016;388:919–931. - PubMed
-
- Verde F, Tredici KD, Braak H, Ludolph A. The multisystem degeneration amyotrophic lateral sclerosis—Neuropathological staging and clinical translation. Arch Ital Biol. 2017;155:118–130. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
