

Patient Perspectives on Psoriatic Disease Burden: Results from the Global Psoriasis and Beyond Survey
- PMID: 37075723
- PMCID: PMC10357389
- DOI: 10.1159/000528945
Patient Perspectives on Psoriatic Disease Burden: Results from the Global Psoriasis and Beyond Survey
Abstract
Background: Patients' understanding of the systemic nature of psoriatic disease (PsD) remains insufficiently explored.
Objectives: The objective of this study was to assess patients' understanding of PsD, associated comorbidities, disease burden, and relationships with healthcare professionals (HCPs).
Methods: Psoriasis and Beyond was a cross-sectional, quantitative online survey conducted in patients with a self-reported, physician-given diagnosis of moderate to severe psoriasis (body surface area [BSA] >5% to <10%, affecting sensitive and/or prominent body parts or BSA ≥10%) at its worst, with/without psoriatic arthritis (PsA). Patients were recruited through online panels by the Institut de Publique Sondage d'Opinion Secteur (Ipsos SA) and patient advocacy groups.
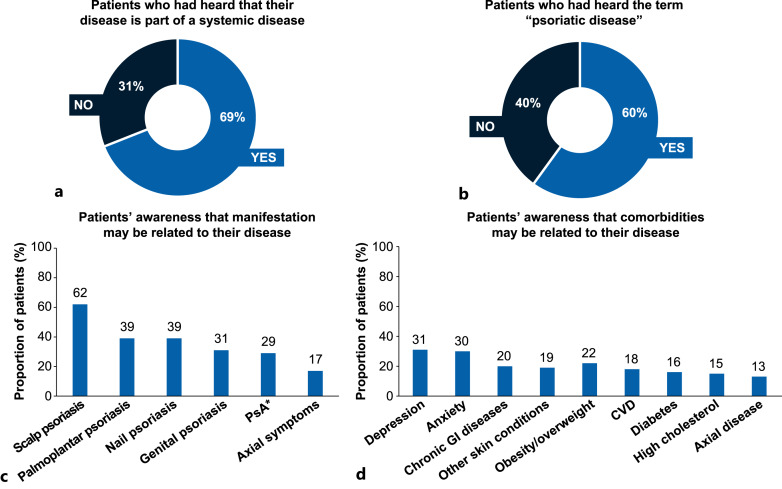
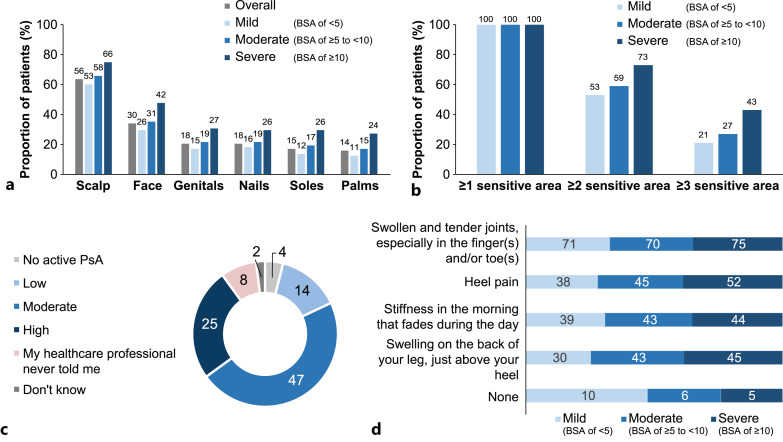
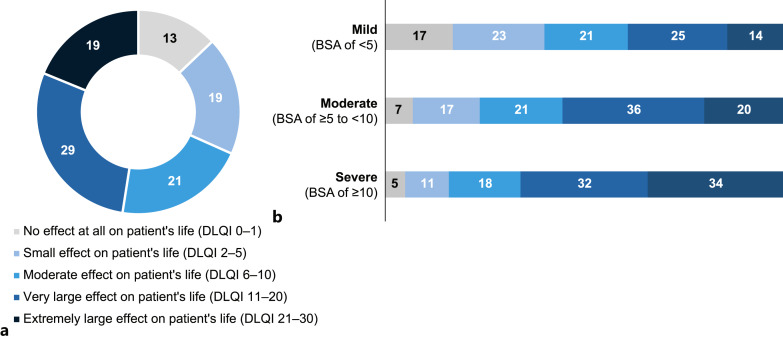
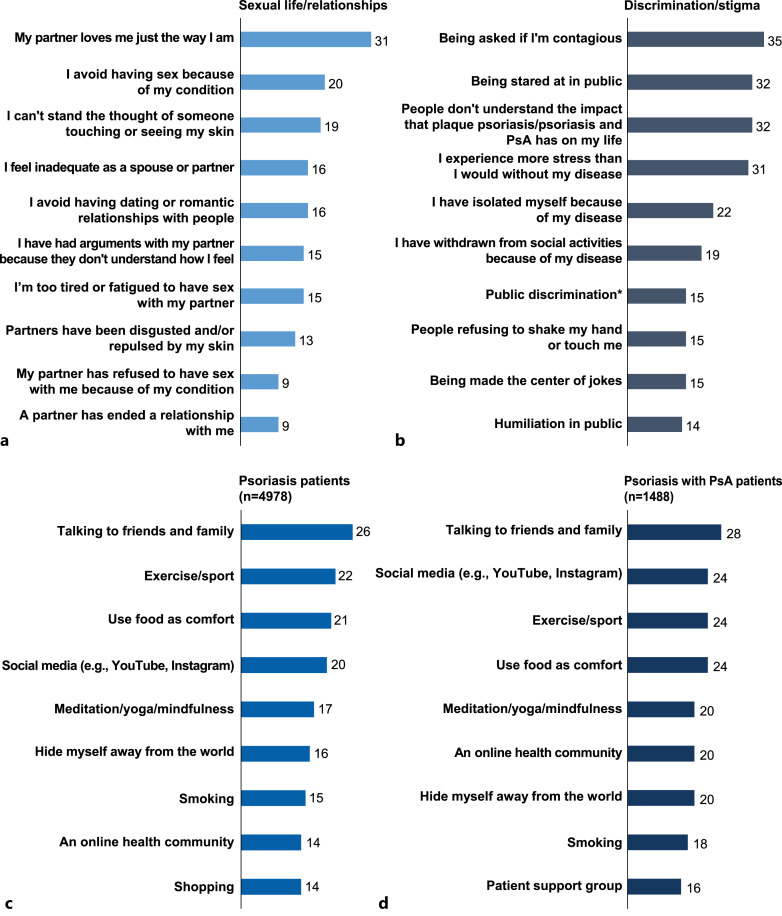
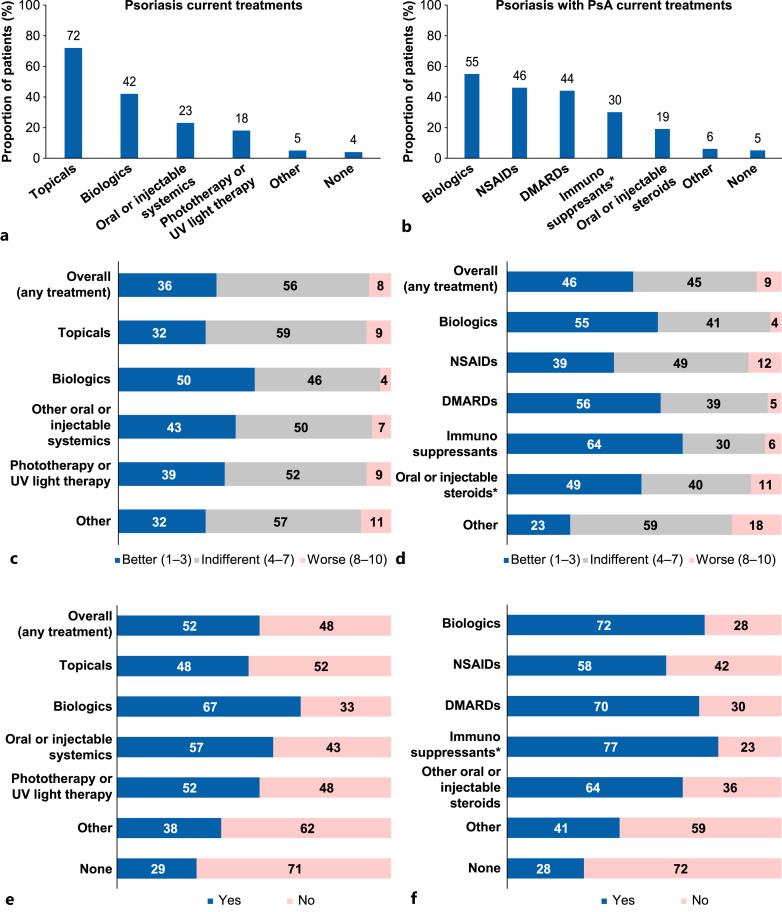
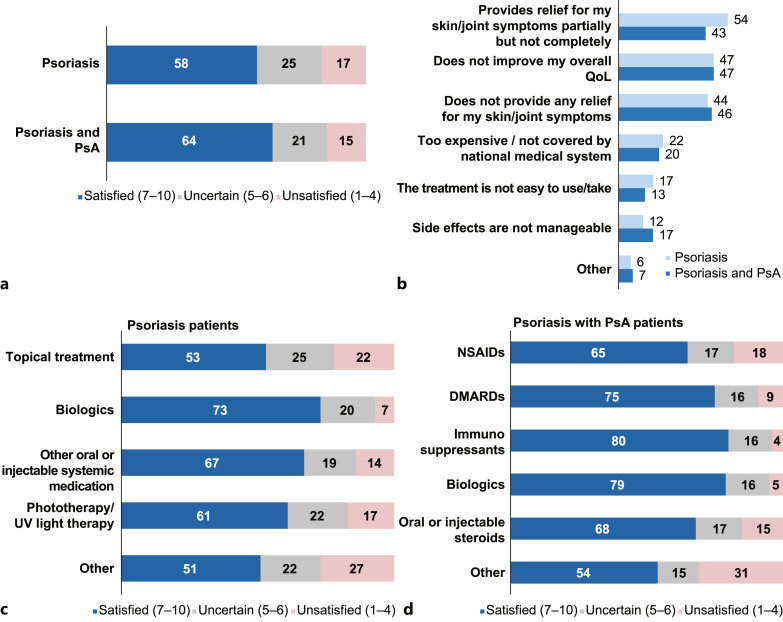
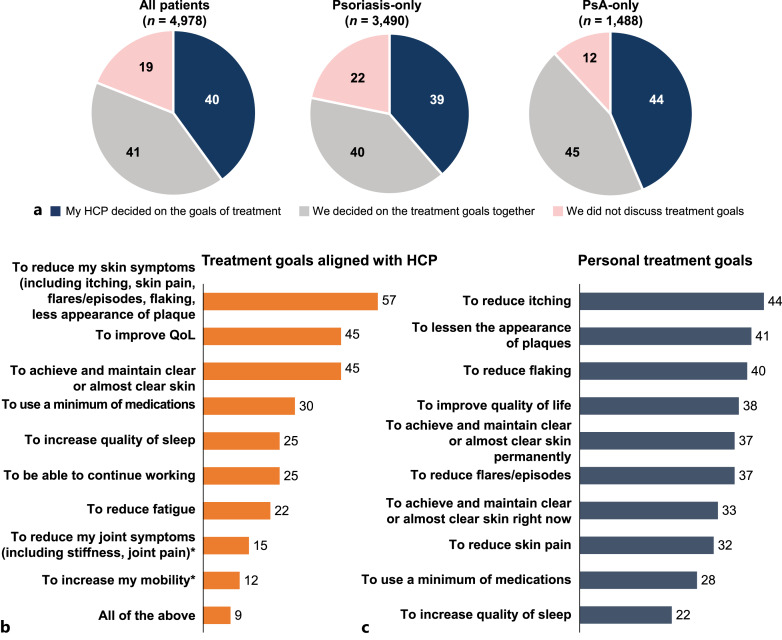
Results: Overall, 4,978 respondents with psoriasis completed the online survey from 20 countries across Australia, Asia, Europe, and the Americas; 30% of patients also reported having concomitant PsA. Overall, 69% of patients with psoriasis had heard that their disease was part of a systemic disease, and 60% had heard of the term "psoriatic disease." Despite this, recognition of common manifestations and comorbidities associated with PsD was low. Among psoriasis-only patients (n = 3,490), 38% screened positive using the Psoriasis Epidemiology Screening Tool (PEST), indicative of potential PsA. Overall, 48% of patients reported that their disease had a very large to extremely large effect on quality of life (QoL; Dermatology Life Quality Index [DLQI] score, 11-30); only 13% of patients reported no impact of the disease on QoL (DLQI, 0-1). Most patients had experienced stigma and discrimination (82%) and a negative impact on relationships (81%) in their lives. Overall, 59% of patients were not involved in deciding their treatment goals: 58% of all treated patients (n = 4,757) and 64% of treated patients with concomitant PsA (n = 1,409) were satisfied with their current treatment.
Conclusions: These results highlight that patients may not fully understand the systemic nature of their disease, were frequently uninvolved in deciding treatment goals, and were often not satisfied with their current treatment. Increasing patients' participation in their care can facilitate shared decision-making between patients and HCPs, which may result in better treatment adherence and patient outcomes. Furthermore, these data indicate that policies should be implemented to protect against stigma and discrimination, which are commonly experienced by patients with psoriasis.
Keywords: Patients’ perspective; Psoriasis; Psoriatic arthritis; Psoriatic disease; Quality of life; Survey; Systemic inflammation.
© 2023 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Figures
References
-
- Lebwohl MG, Kavanaugh A, Armstrong AW, Van Voorhees AS. US perspectives in the management of psoriasis and psoriatic arthritis: patient and physician results from the population-based multinational assessment of psoriasis and psoriatic arthritis (MAPP) survey. Am J Clin Dermatol. 2016 Feb;17(1):87–97. 10.1007/s40257-015-0169-x. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
