

Healthcare utilisation and costs associated with adherence to antipsychotics among people living with HIV/AIDS and schizophrenia: a population-based cohort study in British Columbia, Canada
- PMID: 37076145
- PMCID: PMC10124256
- DOI: 10.1136/bmjopen-2022-070680
Healthcare utilisation and costs associated with adherence to antipsychotics among people living with HIV/AIDS and schizophrenia: a population-based cohort study in British Columbia, Canada
Abstract
Objectives: Non-adherence to antipsychotics is the greatest obstacle to treating schizophrenia. We assessed the economic and clinical impacts of adherence to antipsychotics among people living with HIV/AIDS (PLWH) and schizophrenia in British Columbia, Canada.
Design and setting: A population-based cohort study in British Columbia, Canada.
Methods: Eligible PLWH were enrolled in the Seek and Treat for Optimal Prevention HIV/AIDS population-based cohort during 2001-2016, diagnosed with schizophrenia, on antipsychotics for ≥1 day, and followed for ≥1 year from schizophrenia diagnosis date or 1 January 2001, whichever occurred last.
Primary and secondary outcome measures: A two-part model assessed the marginal effect of adherence on healthcare costs (in 2016 Canadian dollar), while logistic regression examined the effect on virological failure, and generalised linear mixed models examined the effect on hospital readmissions within 30 days and length of hospital stay.
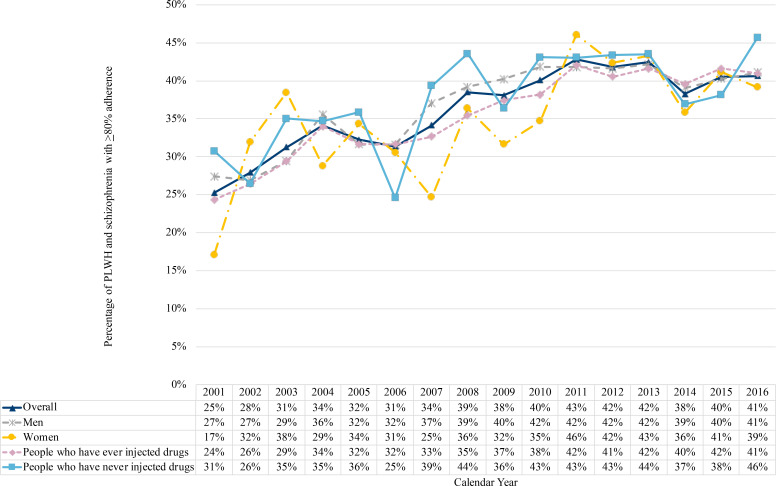
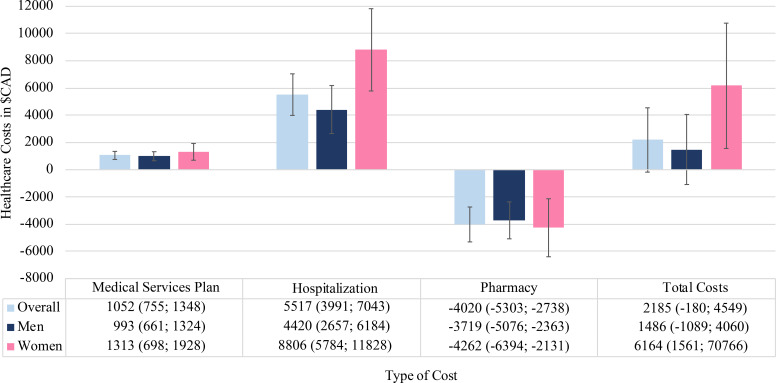
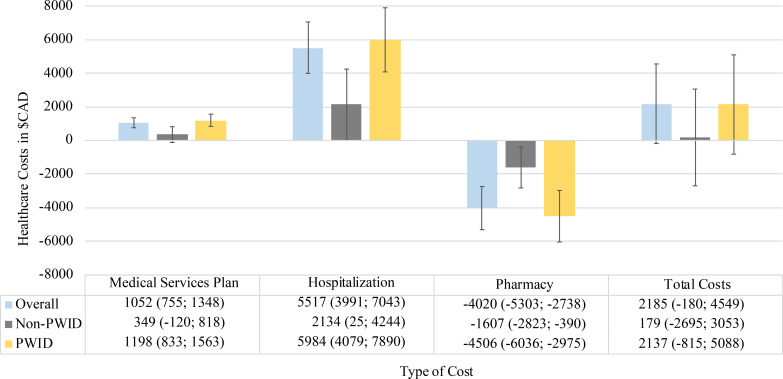
Results: Among 726 PLWH with schizophrenia, ≥80% adherence to antipsychotics increased from 25% (50/198) in 2001 to 41% (225/554) in 2016. In most years, we observed no difference in adherence to antipsychotics among those who used only injectables, only non-injectables, and a combination of both, or among those who have ever consumed typical/first-generation antipsychotics and who consumed only atypical/second-generation antipsychotics. Overall healthcare costs were higher in the non-adherent group ($C2185), driven by the average annual hospitalisation costs ($C5517), particularly among women ($C8806) and people who ever injected drugs (PWID) ($C5985). Non-adherent individuals also experienced higher hospital readmissions (adjusted odds ratio (aOR) 1.48, 95% CI 1.23 to 1.77), and longer hospital stays (adjusted mean ratio 1.23, 95% CI 1.13 to 1.35) in comparison to adherent individuals. We found no difference in virological failure by adherence groups, except when we stratified by gender where the aOR for women was 2.48 (95% CI 1.06 to 5.82).
Conclusions: Our results showed that implementing strategies and interventions to increase antipsychotic adherence, particularly among women and PWID, will be critical in addressing this public health challenge.
Keywords: EPIDEMIOLOGY; HIV & AIDS; PUBLIC HEALTH; Schizophrenia & psychotic disorders; THERAPEUTICS.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JSGM: Institutional grants have been provided by Gilead, Merck and ViiV Healthcare. All other authors declare no competing interests.
Figures
Similar articles
-
Healthcare utilisation in people living with HIV: the role of substance use, mood/anxiety disorders and unsustained viral suppression - a retrospective cohort study in British Columbia, Canada, 2001-2019.BMJ Open. 2025 Mar 5;15(3):e088818. doi: 10.1136/bmjopen-2024-088818. BMJ Open. 2025. PMID: 40044190 Free PMC article.
-
Excess burden of age-associated comorbidities among people living with HIV in British Columbia, Canada: a population-based cohort study.BMJ Open. 2021 Jan 8;11(1):e041734. doi: 10.1136/bmjopen-2020-041734. BMJ Open. 2021. PMID: 33419911 Free PMC article.
-
Factors associated with antiretroviral medication adherence among HIV-positive adults accessing highly active antiretroviral therapy (HAART) in British Columbia, Canada.J Int Assoc Physicians AIDS Care (Chic). 2012 Mar-Apr;11(2):134-41. doi: 10.1177/1545109711423976. Epub 2012 Feb 7. J Int Assoc Physicians AIDS Care (Chic). 2012. PMID: 22318879
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
-
Real-World Evidence of the Clinical and Economic Impact of Long-Acting Injectable Versus Oral Antipsychotics Among Patients with Schizophrenia in the United States: A Systematic Review and Meta-Analysis.CNS Drugs. 2021 May;35(5):469-481. doi: 10.1007/s40263-021-00815-y. Epub 2021 Apr 28. CNS Drugs. 2021. PMID: 33909272 Free PMC article.
Cited by
-
Healthcare utilisation in people living with HIV: the role of substance use, mood/anxiety disorders and unsustained viral suppression - a retrospective cohort study in British Columbia, Canada, 2001-2019.BMJ Open. 2025 Mar 5;15(3):e088818. doi: 10.1136/bmjopen-2024-088818. BMJ Open. 2025. PMID: 40044190 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical