

Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials
- PMID: 37076169
- PMCID: PMC10498296
- DOI: 10.1136/bmj-2022-070730
Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: To investigate the effectiveness and safety of surgery compared with non-surgical treatment for sciatica.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, CINAHL, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, and the World Health Organisation International Clinical Trials Registry Platform from database inception to June 2022.
Eligibility criteria for selecting studies: Randomised controlled trials comparing any surgical treatment with non-surgical treatment, epidural steroid injections, or placebo or sham surgery, in people with sciatica of any duration due to lumbar disc herniation (diagnosed by radiological imaging).
Data extraction and synthesis: Two independent reviewers extracted data. Leg pain and disability were the primary outcomes. Adverse events, back pain, quality of life, and satisfaction with treatment were the secondary outcomes. Pain and disability scores were converted to a scale of 0 (no pain or disability) to 100 (worst pain or disability). Data were pooled using a random effects model. Risk of bias was assessed with the Cochrane Collaboration's tool and certainty of evidence with the grading of recommendations assessment, development, and evaluation (GRADE) framework. Follow-up times were into immediate term (≤six weeks), short term (>six weeks and ≤three months), medium term (>three and <12 months), and long term (at 12 months).
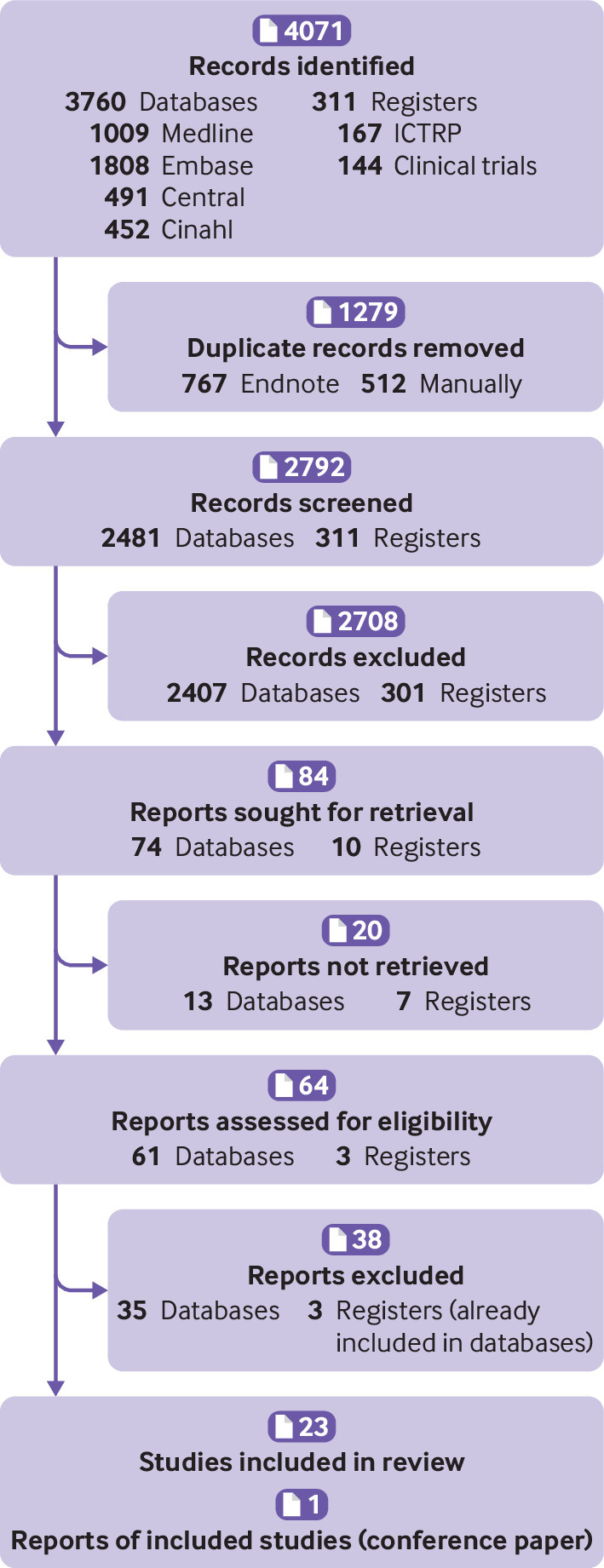
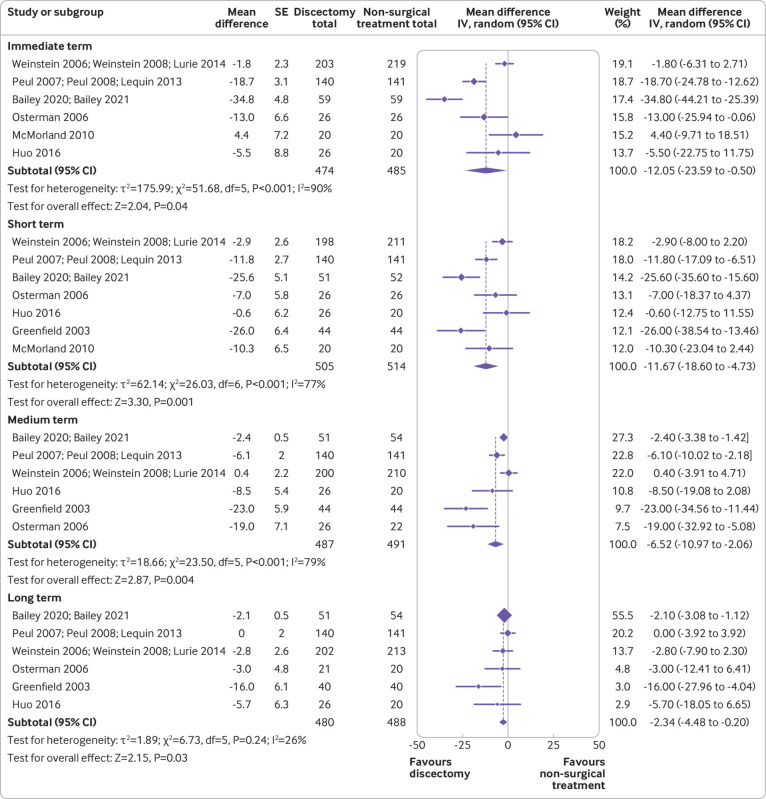
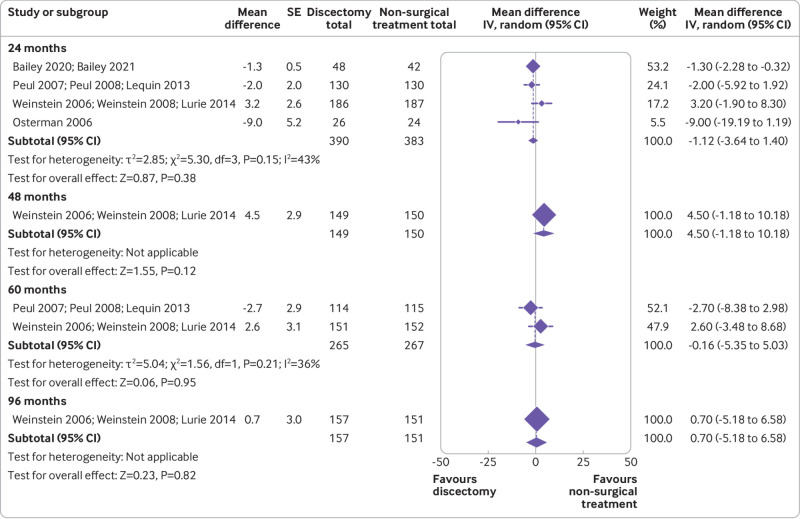
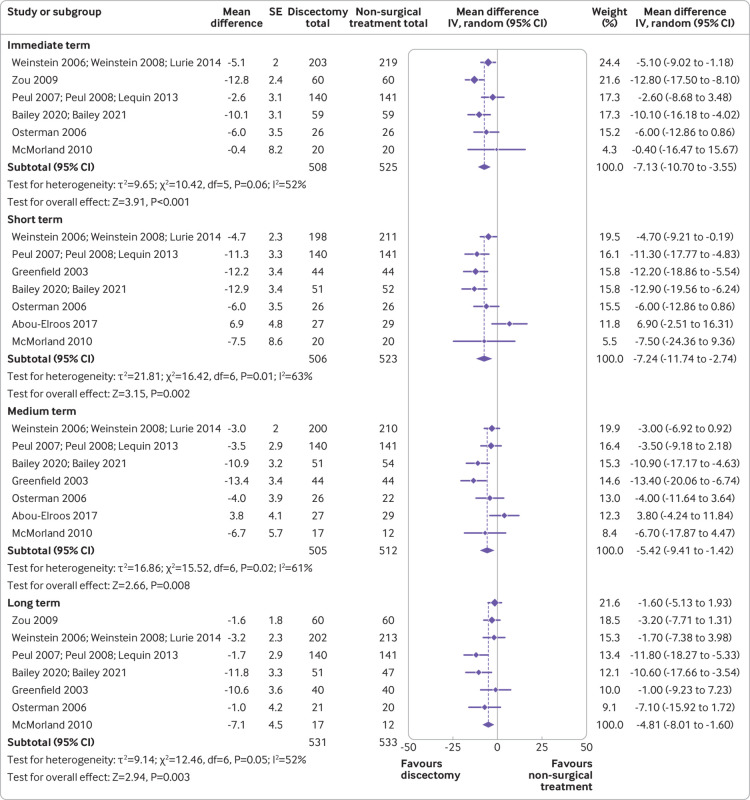
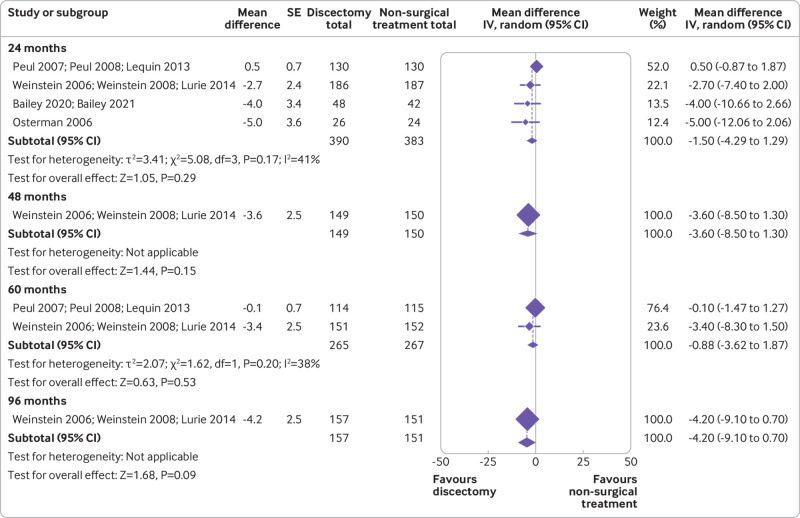
Results: 24 trials were included, half of these investigated the effectiveness of discectomy compared with non-surgical treatment or epidural steroid injections (1711 participants). Very low to low certainty evidence showed that discectomy, compared with non-surgical treatment, reduced leg pain: the effect size was moderate at immediate term (mean difference -12.1 (95% confidence interval -23.6 to -0.5)) and short term (-11.7 (-18.6 to -4.7)), and small at medium term (-6.5 (-11.0 to -2.1)). Negligible effects were noted at long term (-2.3 (-4.5 to -0.2)). For disability, small, negligible, or no effects were found. A similar effect on leg pain was found when comparing discectomy with epidural steroid injections. For disability, a moderate effect was found at short term, but no effect was observed at medium and long term. The risk of any adverse events was similar between discectomy and non-surgical treatment (risk ratio 1.34 (95% confidence interval 0.91 to 1.98)).
Conclusion: Very low to low certainty evidence suggests that discectomy was superior to non-surgical treatment or epidural steroid injections in reducing leg pain and disability in people with sciatica with a surgical indication, but the benefits declined over time. Discectomy might be an option for people with sciatica who feel that the rapid relief offered by discectomy outweighs the risks and costs associated with surgery.
Systematic review registration: PROSPERO CRD42021269997.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. CSB, WCP, and BK report being involved in trials included in the review,5136 and declare that they were not taking any part in assessing that trial in this review.
Figures
Comment in
-
Early surgery for sciatica.BMJ. 2023 Apr 19;381:791. doi: 10.1136/bmj.p791. BMJ. 2023. PMID: 37076178 Free PMC article.
References
-
- Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ 2007;334:1313-7. 10.1136/bmj.39223.428495.BE. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical