

Association of Neighborhood Deprivation With Cognitive and Mood Outcomes in Adults With Pharmacoresistant Temporal Lobe Epilepsy
- PMID: 37076308
- PMCID: PMC10256132
- DOI: 10.1212/WNL.0000000000207266
Association of Neighborhood Deprivation With Cognitive and Mood Outcomes in Adults With Pharmacoresistant Temporal Lobe Epilepsy
Abstract
Background and objectives: Temporal lobe epilepsy (TLE) is the most common adult form of epilepsy and is associated with a high risk of cognitive deficits and depressed mood. However, little is known about the role of environmental factors on cognition and mood in TLE. This cross-sectional study examined the relationship between neighborhood deprivation and neuropsychological function in adults with TLE.
Methods: Neuropsychological data were obtained from a clinical registry of patients with TLE and included measures of intelligence, attention, processing speed, language, executive function, visuospatial skills, verbal/visual memory, depression, and anxiety. Home addresses were used to calculate the Area Deprivation Index (ADI) for each individual, which were separated into quintiles (i.e., quintile 1 = least disadvantaged and quintile 5 = most disadvantaged). Kruskal-Wallis tests compared quintile groups on cognitive domain scores and mood and anxiety scores. Multivariable regression models, with and without ADI, were estimated for overall cognitive phenotype and for mood and anxiety scores.
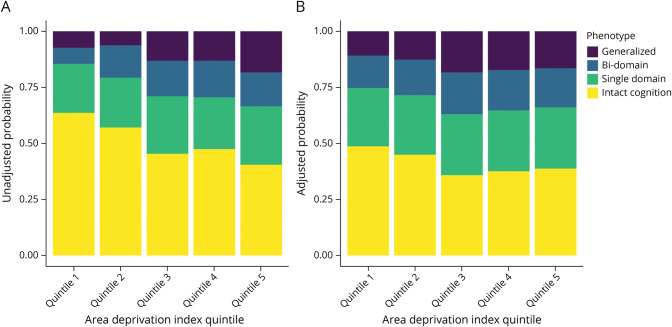
Results: A total of 800 patients (median age 38 years; 58% female) met all inclusion criteria. Effects of disadvantage (increasing ADI) were observed across nearly all measured cognitive domains and with significant increases in symptoms of depression and anxiety. Furthermore, patients in more disadvantaged ADI quintiles had increased odds of a worse cognitive phenotype (p = 0.013). Patients who self-identified as members of minoritized groups were overrepresented in the most disadvantaged ADI quintiles and were 2.91 (95% CI 1.87-4.54) times more likely to be in a severe cognitive phenotype than non-Hispanic White individuals (p < 0.001). However, accounting for ADI attenuated this relationship, suggesting neighborhood deprivation may account for some of the relationship between race/ethnicity and cognitive phenotype (ADI-adjusted proportional odds ratio 1.82, 95% CI 1.37-2.42).
Discussion: These findings highlight the importance of environmental factors and regional characteristics in neuropsychological studies of epilepsy. There are many potential mechanisms by which neighborhood disadvantage can adversely affect cognition (e.g., fewer educational opportunities, limited access to health care, food insecurity/poor nutrition, and greater medical comorbidities). Future research will seek to investigate these potential mechanisms and determine whether structural and functional alterations in the brain moderate the relationship between ADI and cognition.
© 2023 American Academy of Neurology.
Conflict of interest statement
R.M. Busch receives support from the National Institute of Neurological Disorders and Stroke (NINDS) (R01NS120976, R01NS035140, R01NS097719, and R61AG069729). J.E. Dalton receives support from the NIA (R01G055480 and R01AG059979) and NHLBI (R01HL153175). L. Jehi receives support from NINDS (R01NS097719) and NCATS (UL1TR002548). L. Ferguson receives support from the NINDS (R01NS120976, R01NS035140, and R01NS109493). A.F. Struck receives funding from Ceribell. A.F. Struck and B.P. Hermann are supported by the NINDS (R01NS111022, R01NS120976, R01NS117568). None of these grants are directly related to the project reported in this manuscript. Go to
Figures
Comment in
-
The Importance of Understanding Neighborhood Environments in Neurology Care.Neurology. 2023 Jun 6;100(23):1079-1080. doi: 10.1212/WNL.0000000000207390. Epub 2023 Apr 19. Neurology. 2023. PMID: 37076311 Free PMC article. No abstract available.
-
Hiding in Plain Sight-Neighborhood Versus Individual Determinants of Psychological Outcomes in Patients With Epilepsy.Epilepsy Curr. 2024 Jan 23;24(2):102-104. doi: 10.1177/15357597231223588. eCollection 2024 Mar-Apr. Epilepsy Curr. 2024. PMID: 39280052 Free PMC article. No abstract available.
References
-
- Oyegbile TO, Dow C, Jones J, et al. The nature and course of neuropsychological morbidity in chronic temporal lobe epilepsy. Neurology. 2004;62(10):1736-1742. - PubMed
-
- Gilliam FG, Santos J, Vahle V, Carter J, Brown K, Hecimovic H. Depression in epilepsy: ignoring clinical expression of neuronal network dysfunction? Epilepsia. 2004;45(suppl 2):28-33. - PubMed
-
- Tsopelas ND, Saintfort R, Fricchione GL. The relationship of psychiatric illnesses and seizures. Curr Psychiatry Rep. 2001;3:235-242. - PubMed
-
- Giovagnoli AR, Parente A, Tarallo A, Casazza M, Franceschetti S, Avanzini G. Self-rated and assessed cognitive functions in epilepsy: impact on quality of life. Epilepsy Res. 2014;108(8):1461-1468. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous