

CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients With Guillain-Barré Syndrome
- PMID: 37076309
- PMCID: PMC10256127
- DOI: 10.1212/WNL.0000000000207282
CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients With Guillain-Barré Syndrome
Erratum in
-
CSF Findings in Relation to Clinical Characteristics, Subtype, and Disease Course in Patients With Guillain-Barré Syndrome.Neurology. 2023 Sep 26;101(13):592. doi: 10.1212/WNL.0000000000207874. Epub 2023 Aug 29. Neurology. 2023. PMID: 37643890 Free PMC article. No abstract available.
Abstract
Background and objectives: To investigate CSF findings in relation to clinical and electrodiagnostic subtypes, severity, and outcome of Guillain-Barré syndrome (GBS) based on 1,500 patients in the International GBS Outcome Study.
Methods: Albuminocytologic dissociation (ACD) was defined as an increased protein level (>0.45 g/L) in the absence of elevated white cell count (<50 cells/μL). We excluded 124 (8%) patients because of other diagnoses, protocol violation, or insufficient data. The CSF was examined in 1,231 patients (89%).
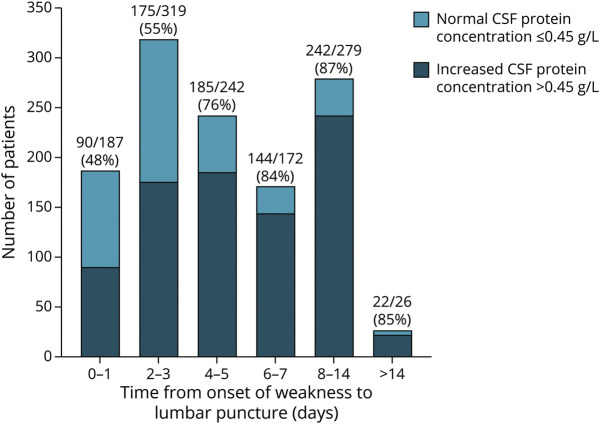
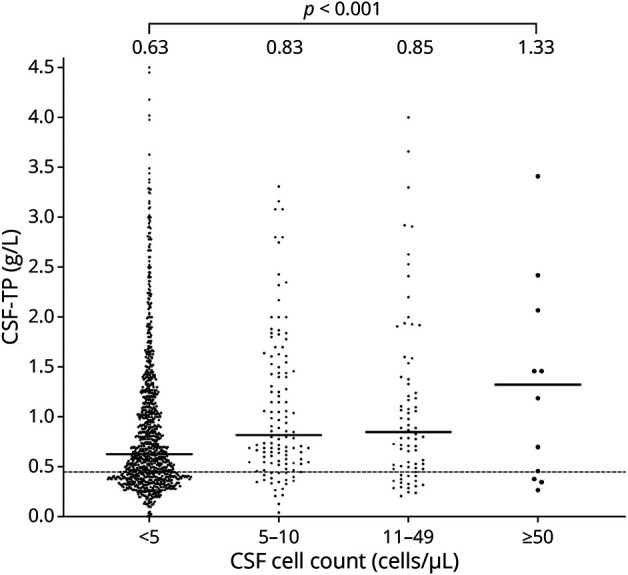
Results: In 846 (70%) patients, CSF examination showed ACD, which increased with time from weakness onset: ≤4 days 57%, >4 days 84%. High CSF protein levels were associated with a demyelinating subtype, proximal or global muscle weakness, and a reduced likelihood of being able to run at week 2 (odds ratio [OR] 0.42, 95% CI 0.25-0.70; p = 0.001) and week 4 (OR 0.44, 95% CI 0.27-0.72; p = 0.001). Patients with the Miller Fisher syndrome, distal predominant weakness, and normal or equivocal nerve conduction studies were more likely to have lower CSF protein levels. CSF cell count was <5 cells/μL in 1,005 patients (83%), 5-49 cells/μL in 200 patients (16%), and ≥50 cells/μL in 13 patients (1%).
Discussion: ACD is a common finding in GBS, but normal protein levels do not exclude this diagnosis. High CSF protein level is associated with an early severe disease course and a demyelinating subtype. Elevated CSF cell count, rarely ≥50 cells/μL, is compatible with GBS after a thorough exclusion of alternative diagnoses.
Classification of evidence: This study provides Class IV evidence that CSF ACD (defined by the Brighton Collaboration) is common in patients with GBS.
© 2023 American Academy of Neurology.
Conflict of interest statement
H. Al-Hakem and A.Y. Doets report no disclosures relevant to the manuscript. A. Stino served on the Scientific Advisory Board for CSL Behring and received research support through Bristol Myers Squibb. S.A. Zivkovic, H. Andersen, and H. Willison report no disclosures relevant to the manuscript. D.R. Cornblath has received consultancy honoraria from Annexon Biosciences, Argenx, Biotest Pharmaceuticals, Cigna Health Management, CSL Behring, DP Clinical, Grifols, Hansa Biopharma, New Enterprise Associates, Octapharma, Pharnext SAS, Polyneuron Pharmaceuticals, Seattle Genetics, Stealth BioTherapeutics, and Syntimmune. David R. Cornblath is also on a data safety monitoring board for Pfizer, Sanofi, Alnylam Pharmaceuticals, PledPharma, and Momenta Pharma. Johns Hopkins University has licensed technology to AstraZeneca Pharmaceuticals, Genentech, Levicept, Seattle Genetics, Merrimack Pharmaceuticals, Levicept, and Disarm Therapeutics, for which David R. Cornblath receives royalties. K.C. Gorson is a consultant for UCB, Pfizer, Annexon, Momenta, and Genentech. Q.D. Mohammad and S.H. Sindrup report no disclosures relevant to the manuscript. S. Kusunoki reports grants from Teijin, grants from Japan Blood Product Organization, grants from Nihon Pharmaceutical, personal fees from Teijin, personal fees from Japan Blood Product Organization, personal fees from Nihon Pharmaceutical, and personal fees from CSL Behring, outside the submitted work. A. Davidson, C. Casasnovas, K. Bateman, J.A.L. Miller, B. van den Berg, C. Verboon, J. Roodbol, S.E. Leonhard, S. Arends, L. Luijten, L. Benedetti. S. Kuwabara, P. Van den Bergh, S. Monges, G.A. Marfia, N. Shahrizaila, G. Galassi, Y. Pereon, J. Bürmann, K. Kuitwaard, R.P. Kleyweg, C. Marchesoni, and M.J. Sedano Tous report no disclosures relevant to the manuscript. L. Querol received research grants from Instituto de Salud Carlos III—Ministry of Economy and Innovation (Spain), GBS-CIDP Foundation International, Novartis Pharma Spain, Roche, UCB and Grifols. L. Querol provided expert testimony to Grifols, CSL Behring, Novartis, Sanofi-Genzyme, Merck, Annexon, Johnson and Johnson, Alexion, UCB, and Roche. Luis Querol serves at Clinical Trial Steering Committee for Sanofi Genzyme and is the principal investigator for UCB’s CIDP01 trial. L. Martín-Aguilar And Y. Wang report no disclosures relevant to the manuscript. E. Nobile-Orazio Eduardo Nobile-Orazio received honorarium for participating in Steering or Advisory Board form Argenx, Belgium; Astellas, the Netherlands; Baxter/Takeda, Italy & USA; CSL Behring, Italy & Switzerland; Janssen, USA; Kedrion, Italy; LFB, France; Novartis, Switzerland; Roche, Switzerland; Sanofi, USA; UCB, UK. He received honorarium for giving lectures from Baxter, USA, & Italy; CSL Behring, Italy; Grifols, Spain; and Kedrion, Italy and travel grants to attend Scientific Meetings from Baxter, Grifols, and Kedrion, Italy. None of these contributions had any relevance for this study. S. Rinaldi, A. Schenone, J. Pardo, F.H. Vermeij, and W. Waheed report no disclosures relevant to the manuscript. H.C. Lehmann reports personal fees from Biogen, CSL Behring, Grifols, Takeda, and Celgene and grants and personal fees from Alnylam and Novartis. V. Granit, B. Stein, G. Cavaletti, G. Gutiérrez-Gutiérrez, F.A. Barroso, L.H. Visser, H.D. Katzberg, E. Dardiotis, S. Attarian, A.J. van der Kooi, P.W. Wirtz, J.P.A. Samijn, and H.J. Gilhuis report no disclosures relevant to the manuscript. R.D.M. Hadden received payments from CSL Behring, Grifols, Argenx, and Alnylam. J.K.L. Holt, K.A. Sheikh, N. Kolb, S. Karafiath, M. Vytopil, G. Antonini, and T.E. Feasby report no disclosures relevant to the manuscript. C.G. Faber reports grants from European Union's Horizon 2020 research and innovation program Marie Sklodowska-Curie grant for PAIN-Net, Molecule-to-man pain network (grant no. 721841), grants from Grifols and Lamepro for a trial on IVIg in small fiber neuropathy, grants from Prinses Beatrix Spierfonds, and Steering committees/advisory board for studies in small fiber neuropathy of Biogen/Convergence, Vertex, Lilly, and OliPass, outside the submitted work. H. Kramers, M. Busby, R.C. Roberts, N.J. Silvestri, R. Fazio, G.W. van Dijk, M.P.J. Garssen, J. Verschuuren, T. Harbo, and B.C. Jacobs report no disclosures relevant to the manuscript. Go to
Figures

Comment in
-
CSF in Guillain-Barré Syndrome: It's a Matter of Timing.Neurology. 2023 Jun 6;100(23):1081-1082. doi: 10.1212/WNL.0000000000207203. Epub 2023 Apr 19. Neurology. 2023. PMID: 37076306 No abstract available.
References
-
- Guillain G, Barre JA, Strohl A. Radiculoneuritis syndrome with hyperalbuminosis of cerebrospinal fluid without cellular reaction. Notes on clinical features and graphs of tendon reflexes. 1916 [in French]. Ann Med Interne (Paris). 1916;150(1):24-32. - PubMed
-
- Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol. 1990;27(suppl):S21-S24. - PubMed
-
- Sejvar JJ, Kohl KS, Gidudu J, et al. Guillain-Barré syndrome and Fisher syndrome: case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine. 2011;29(3):599-612. - PubMed
-
- Hadden RD, Karch H, Hartung HP, et al. Preceding infections, immune factors, and outcome in Guillain-Barré syndrome. Neurology. 2001;56(6):758-765. - PubMed
-
- Haymaker WE, Kernohan JW. The Landry-Guillain-Barré syndrome; a clinicopathologic report of 50 fatal cases and a critique of the literature. Medicine (Baltimore). 1949;28(1):59-141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical