

Corticosteroids in Community-Acquired Bacterial Pneumonia: a Systematic Review, Pairwise and Dose-Response Meta-Analysis
- PMID: 37076606
- PMCID: PMC10115386
- DOI: 10.1007/s11606-023-08203-6
Corticosteroids in Community-Acquired Bacterial Pneumonia: a Systematic Review, Pairwise and Dose-Response Meta-Analysis
Abstract
Introduction: International guidelines provide heterogenous guidance on use of corticosteroids for community-acquired pneumonia (CAP).
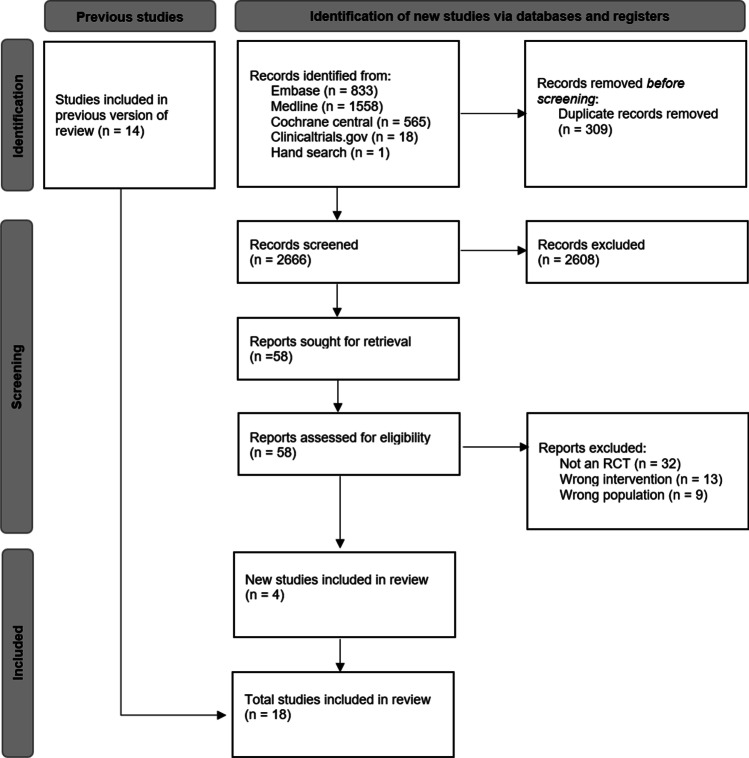
Methods: We performed a systematic review of randomized controlled trials examining corticosteroids in hospitalized adult patients with suspected or probable CAP. We performed a pairwise and dose-response meta-analysis using the restricted maximum likelihood (REML) heterogeneity estimator. We assessed the certainty of the evidence using GRADE methodology and the credibility of subgroups using the ICEMAN tool.
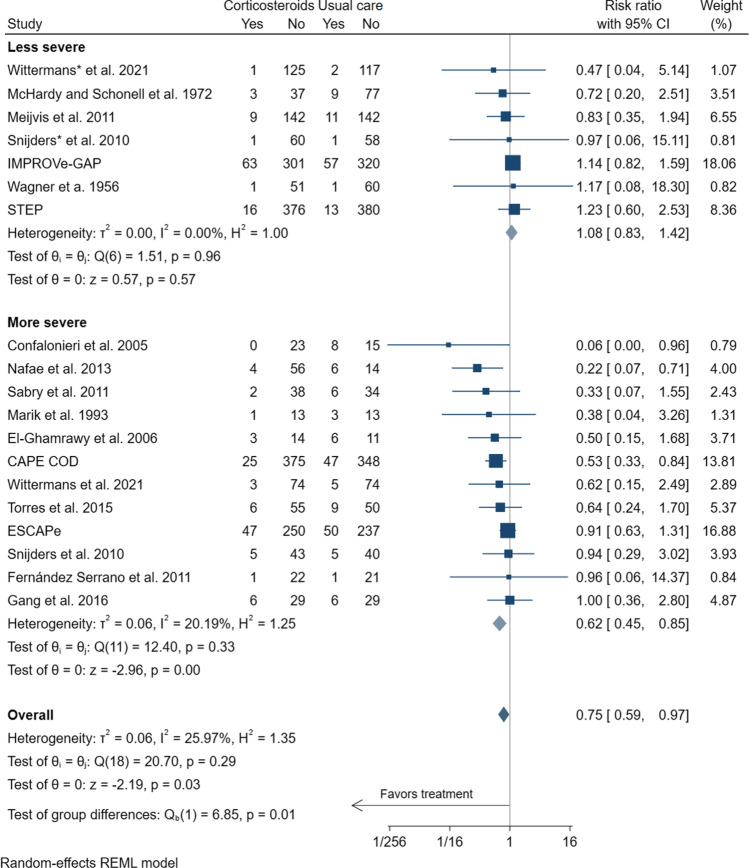
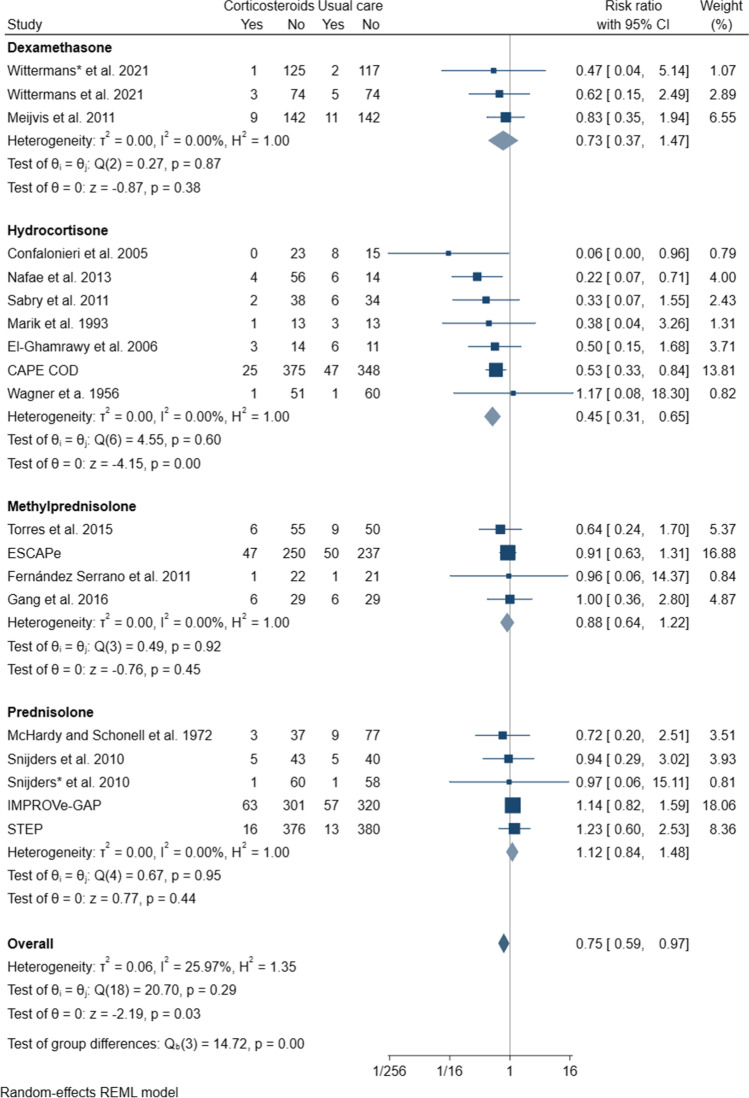
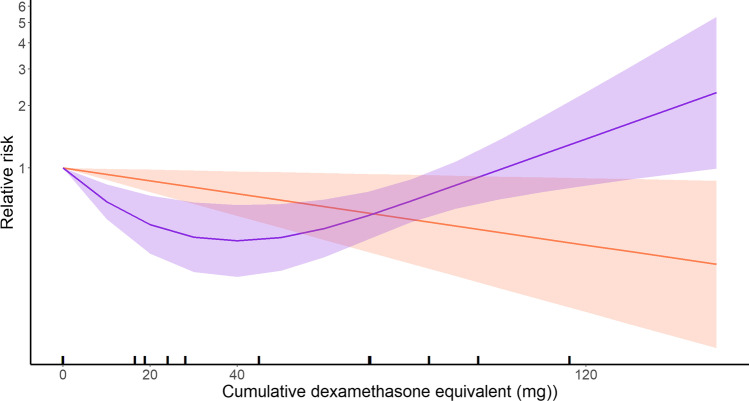
Results: We identified 18 eligible studies that included 4661 patients. Corticosteroids probably reduce mortality in more severe CAP (RR 0.62 [95% CI 0.45 to 0.85]; moderate certainty) with possibly no effect in less severe CAP (RR 1.08 [95% CI 0.83 to 1.42]; low certainty). We found a non-linear dose-response relationship between corticosteroids and mortality, suggesting an optimal dose of approximately 6 mg of dexamethasone (or equivalent) for a duration of therapy of 7 days (RR 0.44 [95% 0.30 to 0.66]). Corticosteroids probably reduce the risk of requiring invasive mechanical ventilation (RR 0.56 [95% CI 0.42 to 74] and probably reduce intensive care unit (ICU) admission (RR 0.65 [95% CI 0.43 to 0.97]) (both moderate certainty). Corticosteroids may reduce the duration of hospitalization and ICU stay (both low certainty). Corticosteroids may increase the risk of hyperglycemia (RR 1.76 [95% CI 1.46 to 2.14]) (low certainty).
Conclusion: Moderate certainty evidence indicates that corticosteroids reduce mortality in patients with more severe CAP, the need for invasive mechanical ventilation, and ICU admission.
© 2023. The Author(s), under exclusive licence to Society of General Internal Medicine.
Conflict of interest statement
TP, DC, SMP, AMN, DN, and BR are members of the Society of Critical Care Medicine Corticosteroid Guidelines Focused Update Panel. SMP is the co-Chair of the Society of Critical Care Medicine Corticosteroid Guidelines Focused Update Panel. SMP discloses personal fees for advisory board work from AbbVie, royalty fees from McGraw Hill as textbook editor, and institutional grant support from the National Cancer Institute of the National Institutes of Health under Award Number P30CA008748, RevImmune, BioMerieux, and the Breast Cancer Research Foundation, outside the submitted work. No other authors made any disclosures.
Figures
Similar articles
-
Corticosteroids in critically ill patients with community-acquired pneumonia: A systematic review and Bayesian meta-analysis.Ann Acad Med Singap. 2024 Nov 18;53(11):683-693. doi: 10.47102/annals-acadmedsg.2024159. Ann Acad Med Singap. 2024. PMID: 39636194
-
Effect of Corticosteroids on Mortality and Clinical Cure in Community-Acquired Pneumonia: A Systematic Review, Meta-analysis, and Meta-regression of Randomized Control Trials.Chest. 2023 Mar;163(3):484-497. doi: 10.1016/j.chest.2022.08.2229. Epub 2022 Sep 7. Chest. 2023. PMID: 36087797 Free PMC article.
-
Comparing the efficacy of corticosteroids among patients with community-acquired pneumonia in the ICU versus non-ICU settings: A systematic review and meta-analysis.Steroids. 2024 May;205:109389. doi: 10.1016/j.steroids.2024.109389. Epub 2024 Feb 13. Steroids. 2024. PMID: 38354995
-
Glucocorticoids can reduce mortality in patients with severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials.Eur J Med Res. 2025 Mar 28;30(1):215. doi: 10.1186/s40001-025-02487-6. Eur J Med Res. 2025. PMID: 40148914 Free PMC article.
-
Corticosteroids in Sepsis and Septic Shock: A Systematic Review, Pairwise, and Dose-Response Meta-Analysis.Crit Care Explor. 2024 Jan 19;6(1):e1000. doi: 10.1097/CCE.0000000000001000. eCollection 2024 Jan. Crit Care Explor. 2024. PMID: 38250247 Free PMC article.
Cited by
-
Best practices for guideline development in Critical Care.Crit Care Sci. 2025 Feb 28;37:e20250372. doi: 10.62675/2965-2774.20250372. eCollection 2025. Crit Care Sci. 2025. PMID: 40053017 Free PMC article. No abstract available.
-
Association of cumulative methylprednisolone dosages with mortality risk from pneumonia in connective tissue disease patients.Sci Rep. 2024 Nov 3;14(1):26502. doi: 10.1038/s41598-024-78233-5. Sci Rep. 2024. PMID: 39489823 Free PMC article.
-
Corticosteroids for adult patients hospitalised with non-viral community-acquired pneumonia: a systematic review and meta-analysis.Intensive Care Med. 2025 May;51(5):917-929. doi: 10.1007/s00134-025-07912-2. Epub 2025 May 5. Intensive Care Med. 2025. PMID: 40323455
-
Updates in Hospital Medicine.J Brown Hosp Med. 2023 Jul 1;2(3):82144. doi: 10.56305/001c.82144. eCollection 2023. J Brown Hosp Med. 2023. PMID: 40026467 Free PMC article. No abstract available.
-
Effect of hydrocortisone on mortality in patients with severe community-acquired pneumonia : The REMAP-CAP Corticosteroid Domain Randomized Clinical Trial.Intensive Care Med. 2025 Apr;51(4):665-680. doi: 10.1007/s00134-025-07861-w. Epub 2025 Apr 22. Intensive Care Med. 2025. PMID: 40261382 Free PMC article. Clinical Trial.
References
-
- Ye Z, Wang Y, Colunga-Lozano LE, Prasad M, Tangamornsuksan W, Rochwerg B, et al. Efficacy and safety of corticosteroids in COVID-19 based on evidence for COVID-19, other coronavirus infections, influenza, community-acquired pneumonia and acute respiratory distress syndrome: a systematic review and meta-analysis. Cmaj. 2020;192(27):E756–e67. - PMC - PubMed
-
- Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Ame J Resp Crit Care Med. 2019;200(7):e45–e67. - PMC - PubMed
-
- Lim WS, Baudouin SV, George RC, Hill AT, Jamieson C, Le Jeune I, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64 Suppl 3:iii1-55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
