

LOREALAUS: LOrlatinib REAL-World AUStralian Experience in Advanced ALK-Rearranged NSCLC
- PMID: 37077199
- PMCID: PMC10106481
- DOI: 10.1016/j.jtocrr.2023.100490
LOREALAUS: LOrlatinib REAL-World AUStralian Experience in Advanced ALK-Rearranged NSCLC
Abstract
Introduction: Over the past decade, ALK tyrosine kinase inhibitors have delivered unprecedented survival for individuals with ALK-positive (ALK+) lung cancers. Real-world data enhance the understanding of optimal drug sequencing and expectations for survival.
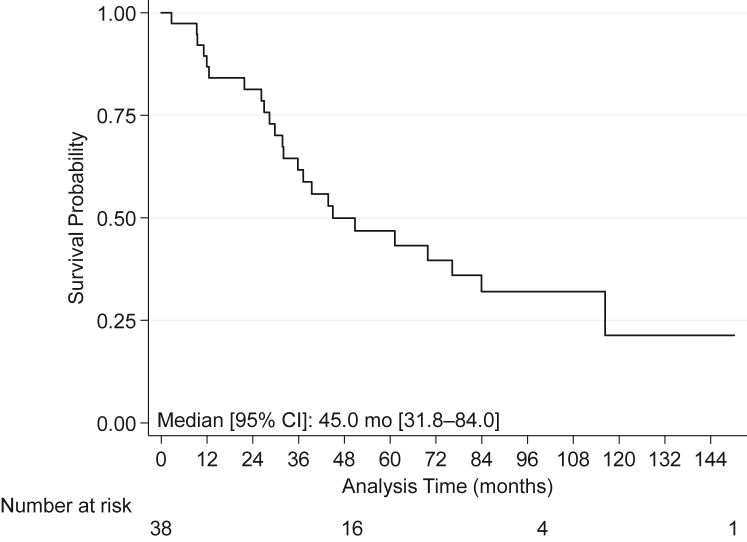
Methods: Multicenter real-world study of individuals with pretreated advanced ALK+ lung cancers managed on a lorlatinib access program between 2016 and 2020. Key outcomes were lorlatinib efficacy, tolerability, and treatment sequencing. Progression-free survival (PFS) and overall survival (OS) were calculated using the Kaplan-Meier method among all individuals (PFSa and OSa), with at least 30 days (one-cycle) lorlatinib exposure (PFSb and OSb), and with good performance status (PFSc and OSc). Subgroups of interest were analyzed to assess signals of potential clinical applicability. Two OS index dates were analyzed, from lorlatinib initiation and advanced ALK+ diagnosis.
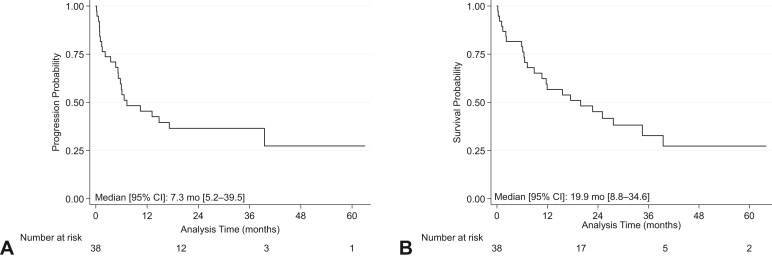
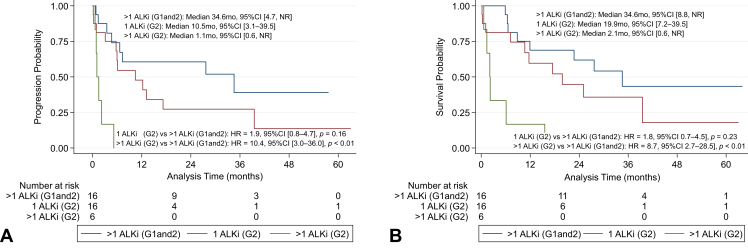
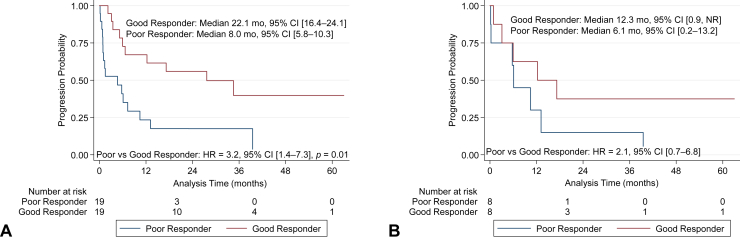
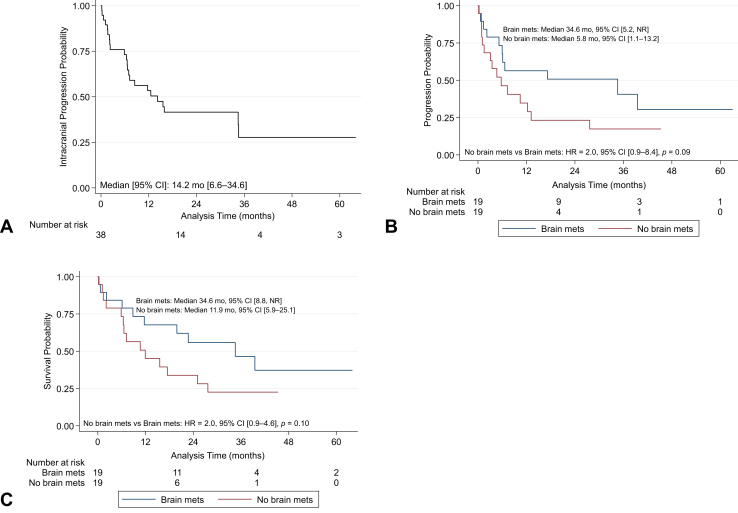
Results: The population (N = 38, 10 sites) was heavily pretreated (23 had ≥2 previous treatment lines) with a high disease burden (26 had 2-4 sites and 11 had >4 sites of metastatic disease, 19 had brain metastases). The overall response rate was 44% and the disease control rate was 81%. Lorlatinib dose reduction (18%), interruption (16%), and discontinuation (3%) were consistent with the trial experience. From advanced ALK+ diagnosis, the median OS for populations a, b, and c was 45.0 months, 69.9 months and 61.2 months respectively. From lorlatinib initiation, the median PFSa, PFSb and PFSc was 7.3 months, 13.2 months and 27.7 months and the median OSa, OSb and OSc was 19.9 months, 25.1 months and 27.7 months. The median PFSa with versus without brain metastases was 34.6 months versus 5.8 months (p = 0.09). The intracranial median PFS was 14.2 months. Previous good response versus poor response to the first ALK-directed therapy median PFSa was 27.7 months versus 4.7 months with a hazard ratio of 0.3 (p = 0.01).
Conclusions: Lorlatinib is a potent, highly active brain-penetrant third-generation ALK tyrosine kinase inhibitors with benefits for most individuals in the later-line setting in a real-world evaluation, consistent with clinical trial data.
Keywords: ALK; Anaplastic Lymphoma Kinase; Lorlatinib; NSCLC; Non–small cell lung cancer; Real-World.
© 2023 The Authors.
Figures

References
-
- Australian Institute of Health and Welfare Cancer in Australia 2021. https://www.aihw.gov.au/reports/cancer/cancer-in-australia-2021/data
-
- John T., Cooper W.A., Wright G., et al. Lung cancer in Australia. J Thorac Oncol. 2020;15:1809–1814. - PubMed
-
- Soda M., Choi Y.L., Enomoto M., et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448:561–566. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
