

Port Site Metastasis After Minimally Invasive Surgery in Gynecologic Malignancies: Two Case Reports and a Review of the Literature
- PMID: 37077283
- PMCID: PMC10106789
- DOI: 10.2147/IJWH.S406488
Port Site Metastasis After Minimally Invasive Surgery in Gynecologic Malignancies: Two Case Reports and a Review of the Literature
Abstract
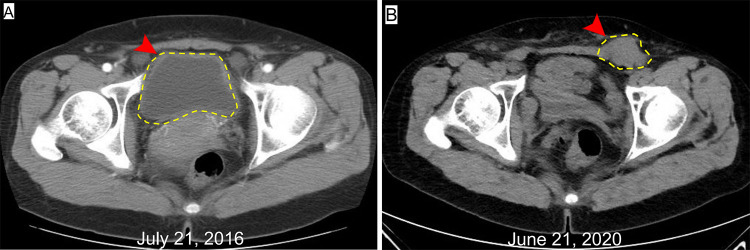
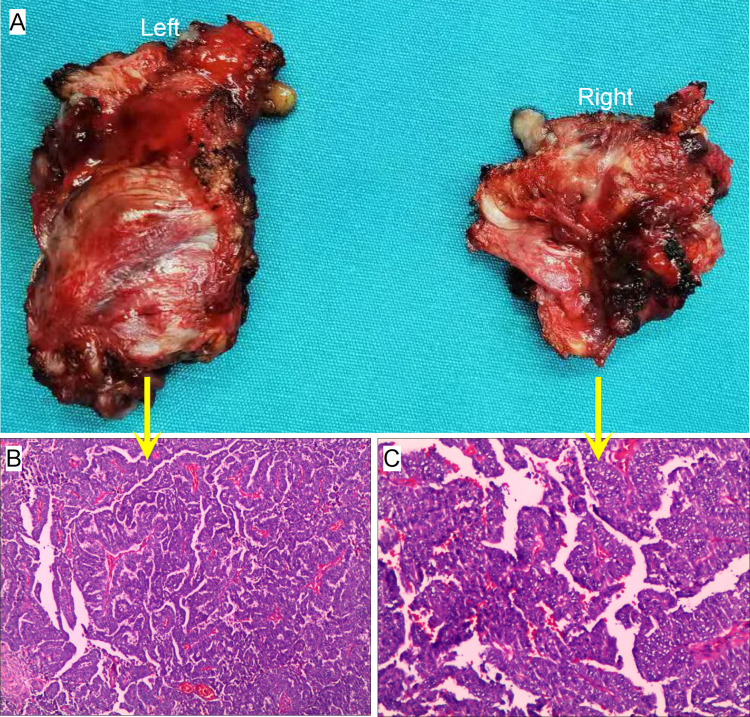
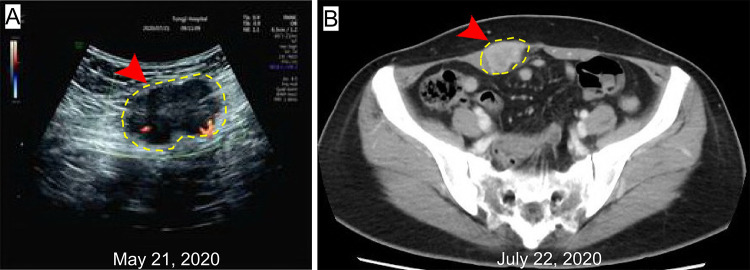
Port site metastasis (PSM) is considered an uncommon and rare complication in gynecologic malignancies with unclear treatment recommendations or guidelines. Thus, we report the treatment strategies and outcomes of two cases of PSMs following gynecologic malignancies and a review of the literature to provide much information about the most frequent sites of PSMs and the incidence of PSMs in different gynecological tumors. A 57-year-old woman underwent laparoscopic radical surgery for right ovarian serous carcinoma in June 2016 followed by postoperative chemotherapy. Because PSMs were present near the port site of the bilateral iliac fossa, the tumors were completely removed on August 4, 2020, and the patient received chemotherapy. She has shown no signs of relapse. During the same period, a 39-year-old woman underwent laparoscopic type II radical hysterectomy for endometrial adenocarcinoma involving the endometrium and cervix on May 4, 2014, without adjuvant treatment. In July 2020, a subcutaneous mass under her abdominal incision was removed, and chemotherapy plus radiotherapy was administered. Metastasis was found in the left lung in September 2022, but there was no abnormality in the abdominal incision. We showed the two cases of PSMs, reviewed articles to provide some new insights about the incidences of PSMs in the gynecologic tumors, and discussed the proper preventive strategies.
Keywords: endometrial cancer; metastasis; ovarian cancer; port site.
© 2023 Yu et al.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Port-Site Metastasis in Gynecological Malignancies.JSLS. 2021 Jan-Mar;25(1):e2020.00081. doi: 10.4293/JSLS.2020.00081. JSLS. 2021. PMID: 33879998 Free PMC article. Review.
-
Isolated port-site metastasis after surgical staging for low-risk endometrioid endometrial cancer: A case report.Oncol Lett. 2016 Jul;12(1):281-284. doi: 10.3892/ol.2016.4595. Epub 2016 May 17. Oncol Lett. 2016. PMID: 27347138 Free PMC article.
-
Port site metastases a year after initial laparoscopic cholecystectomy. Should the use of retrieval bags during laparoscopic cholecystectomy be the new gold standard?Pol Przegl Chir. 2021 May 31;93(6):61-65. doi: 10.5604/01.3001.0015.3280. Pol Przegl Chir. 2021. PMID: 36169533
-
Abdominal wall port site metastasis after robotically staged endometrial carcinoma: A case report.Int J Surg Case Rep. 2013;4(7):613-5. doi: 10.1016/j.ijscr.2013.04.006. Epub 2013 Apr 18. Int J Surg Case Rep. 2013. PMID: 23708308 Free PMC article.
-
Port site metastasis after robotic-assisted laparoscopic hysterectomy for uterine cervical cancer: a case report and literature review.Taiwan J Obstet Gynecol. 2013 Dec;52(4):558-63. doi: 10.1016/j.tjog.2013.10.018. Taiwan J Obstet Gynecol. 2013. PMID: 24411043 Review.
Cited by
-
The minimally invasive resection of port-site metastasis of ovarian cancer after laparoscopy with cutaneous integrity: a case report and literature review.BMC Womens Health. 2024 Sep 6;24(1):494. doi: 10.1186/s12905-024-03353-z. BMC Womens Health. 2024. PMID: 39242540 Free PMC article. Review.
References
-
- Kadar N. Port-site recurrences following laparoscopic operations for gynaecological malignancies. Br J Obstet Gynaecol. 1997;104(11):1308–1313. - PubMed
-
- Ramirez PT, Frumovitz M. Wolf JK and Levenback C. Laparoscopic port-site metastases in patients with gynecological malignancies. Int J Gynecol Cancer. 2004;14(6):1070–1077. - PubMed
-
- Kim B, Huh SJ, Kim BG. Port site metastasis after robotic-assisted laparoscopic hysterectomy for uterine cervical cancer: a case report and literature review. Taiwan J Obstet Gynecol. 2013;52(4):558–563. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
