

A National Implementation Project to Prevent Healthcare-Associated Infections in Intensive Care Units: A Collaborative Initiative Using the Breakthrough Series Model
- PMID: 37077504
- PMCID: PMC10109530
- DOI: 10.1093/ofid/ofad129
A National Implementation Project to Prevent Healthcare-Associated Infections in Intensive Care Units: A Collaborative Initiative Using the Breakthrough Series Model
Abstract
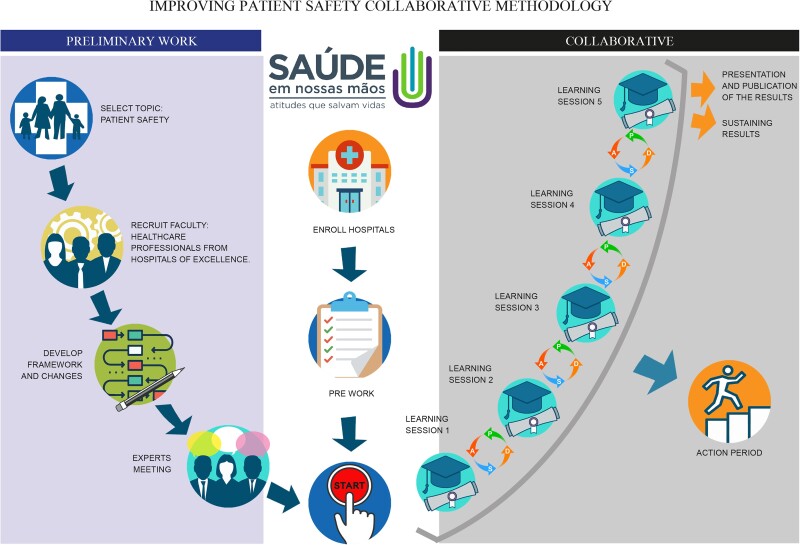
Background: Although there are simple and low-cost measures to prevent healthcare-associated infections (HAIs), they remain a major public health problem. Quality issues and a lack of knowledge about HAI control among healthcare professionals may contribute to this scenario. In this study, our aim is to present the implementation of a project to prevent HAIs in intensive care units (ICUs) using the quality improvement (QI) collaborative model Breakthrough Series (BTS).
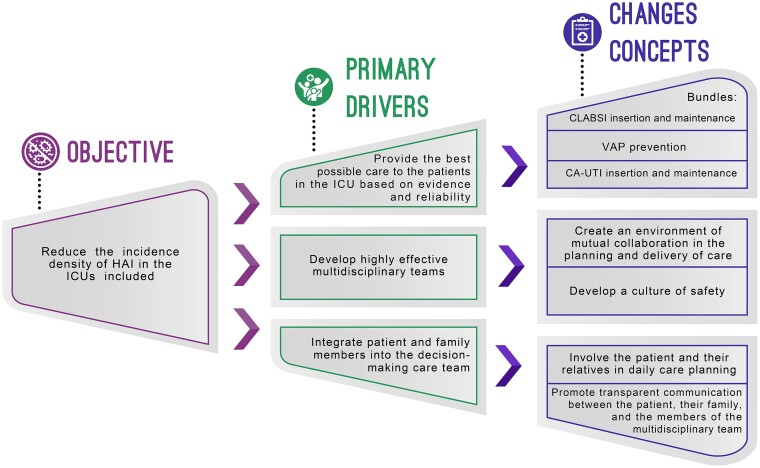
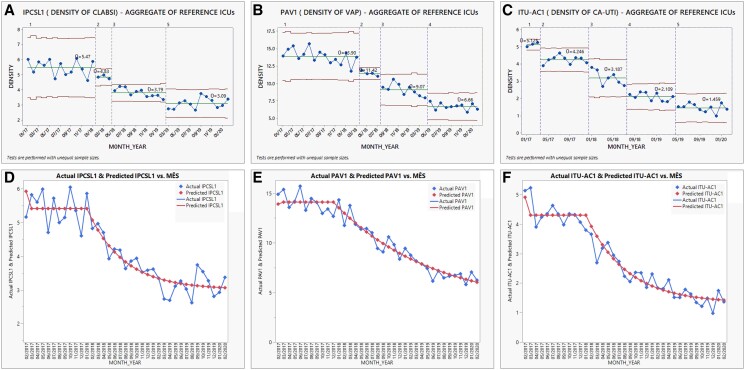
Methods: A QI report was conducted to assess the results of a national project in Brazil between January 2018 and February 2020. A 1-year preintervention analysis was conducted to determine the incidence density baseline of the 3 main HAIs: central line-associated bloodstream infections (CLABSIs), ventilation-associated pneumonia (VAP), and catheter-associated urinary tract infections (CA-UTIs). The BTS methodology was applied during the intervention period to coach and empower healthcare professionals providing evidence-based, structured, systematic, and auditable methodologies and QI tools to improve patients' care outcomes.
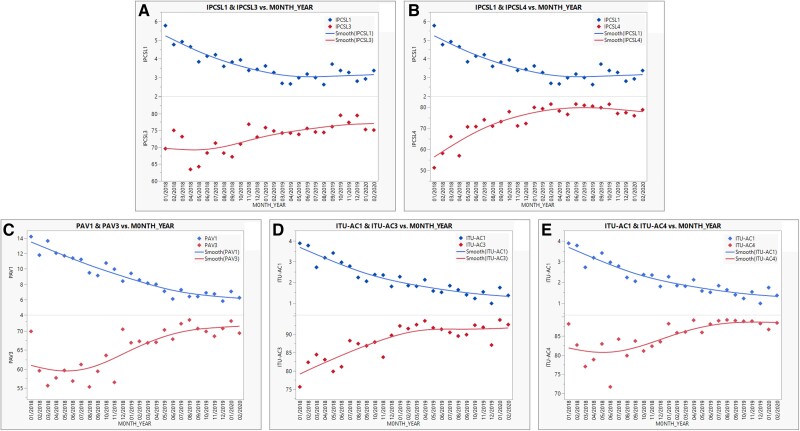
Results: A total of 116 ICUs were included in this study. The 3 HAIs showed a significant decrease of 43.5%, 52.1%, and 65.8% for CLABSI, VAP, and CA-UTI, respectively. A total of 5140 infections were prevented. Adherence to bundles inversely correlated with the HAI incidence densities: CLABSI insertion and maintenance bundle (R = -0.50, P = .010 and R = -0.85, P < .001, respectively), VAP prevention bundle (R = -0.69, P < .001), and CA-UTI insertion and maintenance bundle (R = -0.82, P < .001 and R = -0.54, P = .004, respectively).
Conclusions: Descriptive data from the evaluation of this project show that the BTS methodology is a feasible and promising approach to preventing HAIs in critical care settings.
Keywords: central line-associated bloodstream infection; healthcare-associated infection; quality improvement; urinary tract infection; ventilator-associated pneumonia.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts of interest.
Figures
References
-
- Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008; 36:309–32. - PubMed
-
- Rosenthal VD, Duszynska W, Ider BE, et al. . International Nosocomial Infection Control Consortium (INICC) report, data summary of 45 countries for 2013–2018, adult and pediatric units, device-associated module. Am J Infect Control 2021; 49:1267–74. - PubMed
-
- Allegranzi B, Nejad SB, Combescure C, et al. . Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011; 377:228–41. - PubMed
