

The thoracolumbar interfascial block with local anesthesia in osteoporotic vertebral compression fractures treated with percutaneous kyphoplasty provides better analgesia compared with local anesthesia alone: A randomized controlled study
- PMID: 37077867
- PMCID: PMC10106675
- DOI: 10.3389/fsurg.2023.1133637
The thoracolumbar interfascial block with local anesthesia in osteoporotic vertebral compression fractures treated with percutaneous kyphoplasty provides better analgesia compared with local anesthesia alone: A randomized controlled study
Abstract
Objective: To evaluate the safety and efficacy of the thoracolumbar interfascial block (TLIPB) in percutaneous kyphoplasty (PKP), and to confirm that the TLIPB further minimizes perioperative pain and residual back pain on the basis of local anesthesia.
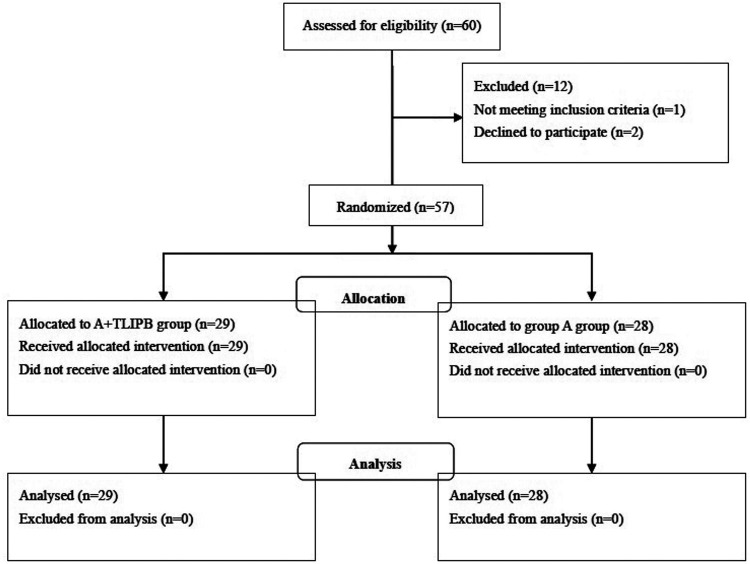
Method: From April 2021 to May 2022, 60 patients with osteoporotic vertebral compression fractures were included in this prospective randomized controlled trial. Patients were randomly assigned to a local anesthesia group (A group) or a TLIPB on the basis of local anesthesia group (A + TLIPB group) before PKP. Pain level (visual analog scale, VAS), amount of analgesic rescue drugs (parecoxib), operative time, mean arterial pressure, heart rate, and complications were assessed and compared between the two groups.
Results: Compared with the A group, VAS scores were lower in the A + TLIPB group, respectively, when the trocar punctured the vertebral body (7.4 ± 0.7 vs. 4.5 ± 0.9; P < 0.01), during balloon dilatation (6.6 ± 0.9 vs. 4.6 ± 0.9; P < 0.01), during bone cement injection (6.3 ± 0.6 vs. 4.3 ± 0.8; P < 0.01), 1 h after surgery (3.5 ± 0.7 vs. 2.9 ± 0.7; P < 0.01), and 24 h after surgery (2.5 ± 0.8 vs. 1.9 ± 0.4; P < 0.01). Residual back pain (VAS: 1.9 ± 0.9 vs. 0.9 ± 0.8; P < 0.01) and the incidence of rescue analgesic use (P = 0.02) in the A + TLIPB group were lower compared with the A group. Compared with the A group, mean arterial pressure and heart rate were lower in the A + TLIPB group when the trocar punctured the vertebral body, and with balloon dilatation and bone cement injection; however, there were no statistical differences between the groups 1 and 24 h after surgery. The incidences of bone cement leakage, constipation, and nausea were similar between the two groups. No patient developed infection, neurological injuries, constipation in either group.
Conclusion: The addition of the TLIPB to local anesthesia can further minimize perioperative pain and residual back pain, and reduce perioperative rescue analgesic use. When added to local anesthesia, the TLIPB is an effective and safe anesthetic method for PKP.
Clinical trial registration: This study has been registered in the Clinical Trial registration: ChiCTR-2100044236.
Keywords: elderly patients; osteoporotic vertebral compression fractures; pain management; percutaneous kyphoplasty; thoracolumbar interfascial block.
© 2023 Tao, Zhang, Jiang, Fan, Wang and Zheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Comparison of percutaneous balloon dilation kyphoplasty and percutaneous vertebroplasty in treatment for thoracolumbar vertebral compression fractures.Eur Rev Med Pharmacol Sci. 2018 Jul;22(1 Suppl):96-102. doi: 10.26355/eurrev_201807_15370. Eur Rev Med Pharmacol Sci. 2018. PMID: 30004560
-
Comparative evaluation of an innovative deflectable percutaneous kyphoplasty versus conventional bilateral percutaneous kyphoplasty for osteoporotic vertebral compression fractures: a prospective, randomized and controlled trial.Spine J. 2023 Apr;23(4):585-598. doi: 10.1016/j.spinee.2022.12.012. Epub 2022 Dec 20. Spine J. 2023. PMID: 36563860 Clinical Trial.
-
Balloon kyphoplasty: an evidence-based analysis.Ont Health Technol Assess Ser. 2004;4(12):1-45. Epub 2004 Dec 1. Ont Health Technol Assess Ser. 2004. PMID: 23074451 Free PMC article.
-
Can Additional Facet Joint Block Improve the Clinical Outcome of Kyphoplasty for Acute Osteoporotic Vertebral Compression Fractures?Pain Physician. 2021 May;24(3):283-291. Pain Physician. 2021. PMID: 33988948
-
Comparison of Percutaneous Vertebroplasty and Balloon Kyphoplasty for the Treatment of Single Level Vertebral Compression Fractures: A Meta-analysis of the Literature.Pain Physician. 2015 May-Jun;18(3):209-22. Pain Physician. 2015. PMID: 26000665 Review.
Cited by
-
Risk factors of residual back pain after vertebral augmentation in osteoporotic vertebral compression fracture patients: a systematic review and meta-analysis.BMC Musculoskelet Disord. 2025 Jul 25;26(1):702. doi: 10.1186/s12891-025-08945-w. BMC Musculoskelet Disord. 2025. PMID: 40713499 Free PMC article.
References
-
- Melton LJ, Cooper C. Magnitude and impact of osteoporosis and fractures. In: Osteoporosis Vol. 1. 2nd ed. Edited by Marcus R, Feldman D, Kelsey J. San Diego CA: Academic Press; (2001). p. 557–67.
-
- Xu JJ, Tang XT, Yang J, Wang YH, Zhu DC, Wu Ys, et al. The effect of medial branch block on postoperative residual pain relieve after percutaneous kyphoplasty: a randomized controlled trial with 12-month follow-up. Pain Physician. (2021) 24(7):E1059–66. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous