

Concomitance of Hidradenitis Suppurativa and Porokeratoses
- PMID: 37077926
- PMCID: PMC10110287
Concomitance of Hidradenitis Suppurativa and Porokeratoses
Abstract
Objective: No known studies have attempted to describe the pathophysiological relationship between patients who develop both porokeratosis and hidradenitis suppurativa (HS). The purpose of this report is to present possible immunological mechanisms that predispose patients to developing both porokeratosis and HS.
Methods: In this case series, patients were identified during routine clinical encounters and data was extracted from the electronic medical record from October 2010 until April 2021. This study is a single center case series including patients from the department of dermatology at the UNC School of Medicine in Chapel Hill, North Carolina. Patients were selected via digital chart review if they had simultaneous diagnoses of disseminated porokeratosis and HS. Two eligible patients were identified as actively receiving care. One patient is a Black female and the other a White male. No primary study outcomes were planned. This investigation utilized chart review to identify disease time course, which was subsequently used to elucidate study outcomes.
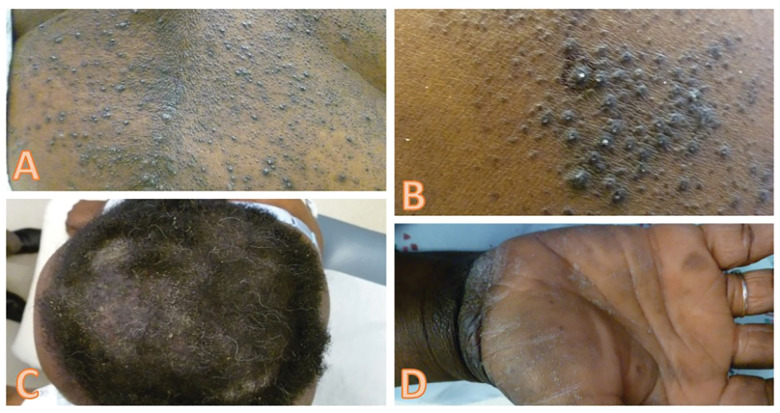
Results: Patient A is a 54-year-old Black female and Patient B is a 65-year-old White male. Both patients developed porokeratosis after multiple years of living with HS. Immunosuppression with adalimumab, corticosteroids, or other medications did not clearly precede porokeratosis development in either patient.
Limitations: Limitations include that this study was conducted at a single center and prevalence of patients with concomitance of both conditions is low.
Conclusion: In patients who demonstrate simultaneous HS and porokeratosis, activation of the innate immune system and associated IL-1 production may lead to autoinflammation and a phenotype of hyperkeratinization. Mutations in genes such as mevalonate kinase may predispose subjects to the development of porokeratoses and HS.
Keywords: Hidradenitis suppurativa; interleukin-1 (IL-1); porokeratoses; porokeratosis.
Copyright © 2023. Matrix Medical Communications. All rights reserved.
Conflict of interest statement
DISCLOSURES: The authors report no conflicts on interest relevant to the content of this article.
Figures


References
-
- Chernosky ME. Porokeratosis. Arch Dermatol. 1986;122(8):869–870. - PubMed
-
- Alikhan A et al. North American clinical management guidelines for hidradenitis suppurativa: A publication from the United States and Canadian Hidradenitis Suppurativa Foundations: Part I: Diagnosis, evaluation, and the use of complementary and procedural management. J Am Acad Dermatol. 2019;81(1):76–90. - PMC - PubMed
-
- Smith J et al. Brachytherapy for Resistant Disseminated Superficial Actinic Porokeratosis. Applied Radiation Oncology. 2020;9(3):p. 43–45.
-
- Young PM et al. An unusual spiculated presentation of follicular porokeratosis. Dermatol Online J. 2019;25(7) - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous