

Lipoprotein(a) and calcific aortic valve disease initiation and progression: a systematic review and meta-analysis
- PMID: 37078819
- PMCID: PMC10702855
- DOI: 10.1093/cvr/cvad062
Lipoprotein(a) and calcific aortic valve disease initiation and progression: a systematic review and meta-analysis
Abstract
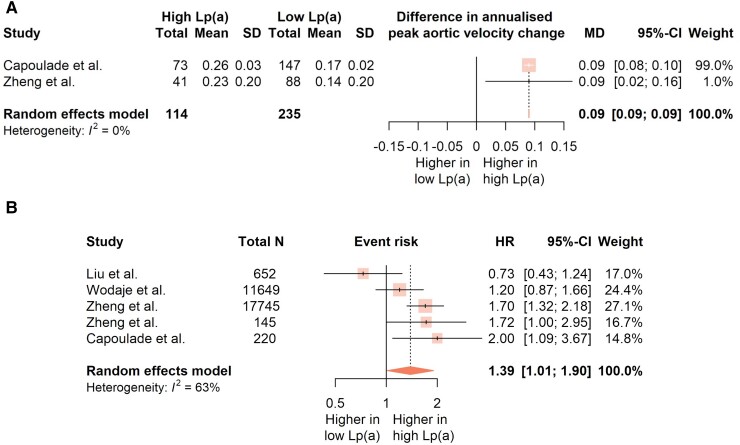
Although evidence indicates the association of lipoprotein(a) [Lp(a)] with atherosclerosis, the link with calcific aortic valve disease (CAVD) is unclear. This systematic review and meta-analysis explores the connection between Lp(a) and aortic valve calcification and stenosis (AVS). We included all relevant studies, indexed in eight databases, up to February 2023. A total of 44 studies (163 139 subjects) were included, with 16 of them being further meta-analysed. Despite considerable heterogeneity, most studies support the relationship between Lp(a) and CAVD, especially in younger populations, with evidence of early aortic valve micro-calcification in elevated-Lp(a) populations. The quantitative synthesis showed higher Lp(a) levels, by 22.63 nmol/L (95% CI: 9.98-35.27), for patients with AVS, while meta-regressing the data revealed smaller Lp(a) differences for older populations with a higher proportion of females. The meta-analysis of eight studies providing genetic data, revealed that the minor alleles of both rs10455872 and rs3798220 LPA gene loci were associated with higher risk for AVS (pooled odds ratio 1.42; 95% CI: 1.34-1.50 and 1.27; 95% CI: 1.09-1.48, respectively). Importantly, high-Lp(a) individuals displayed not only faster AVS progression, by a mean difference of 0.09 m/s/year (95% CI: 0.09-0.09), but also a higher risk of serious adverse outcomes, including death (pooled hazard ratio 1.39; 95% CI: 1.01-1.90). These summary findings highlight the effect of Lp(a) on CAVD initiation, progression and outcomes, and support the early onset of Lp(a)-related subclinical lesions before clinical evidence.
Keywords: Aortic valve stenosis; Calcific aortic valve disease; Lipoprotein(a); Lp(a); Meta-analysis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: None declared.
Figures




References
-
- Levine GN. Cardiology secrets. 5th ed. Philadelphia, PA: Elsevier; 2018. p269–276.
-
- Chan K-L. Lipoprotein(a) and aortic stenosis. Heart 2022;108:9–10. - PubMed
-
- Tsimikas S. A test in context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol 2017;69:692–711. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Miscellaneous
