

Validating real-time three-dimensional echocardiography against cardiac magnetic resonance, for the determination of ventricular mass, volume and ejection fraction: a meta-analysis
- PMID: 37079054
- PMCID: PMC10881629
- DOI: 10.1007/s00392-023-02204-5
Validating real-time three-dimensional echocardiography against cardiac magnetic resonance, for the determination of ventricular mass, volume and ejection fraction: a meta-analysis
Abstract
Introduction: Real-time three-dimensional echocardiography (RT3DE) is currently being developed to overcome the challenges of two-dimensional echocardiography, as it is a much cheaper alternative to the gold standard imaging method, cardiac magnetic resonance (CMR). The aim of this meta-analysis is to validate RT3DE by comparing it to CMR, to ascertain whether it is a practical imaging method for routine clinical use.
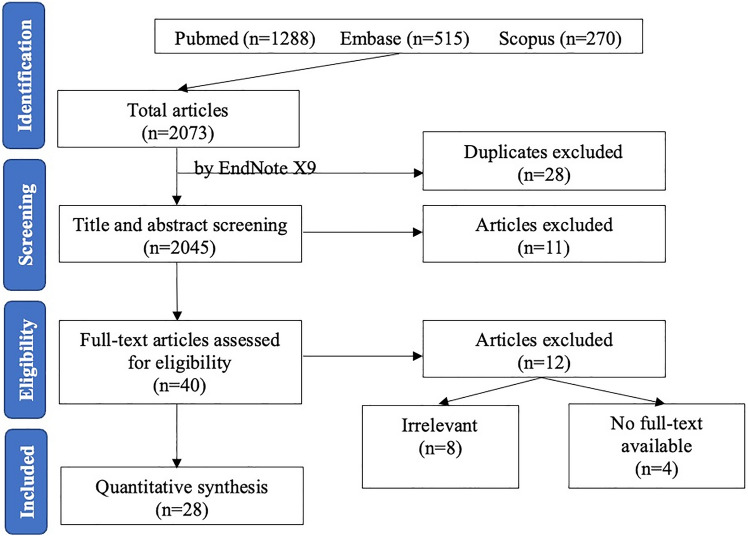
Methods: A systematic review and meta-analysis method was used to synthesise the evidence and studies published between 2000 and 2021 were searched using a PRISMA approach. Study outcomes included left ventricular end-systolic volume (LVESV), left ventricular end-diastolic volume (LVEDV), left ventricular ejection fraction (LVEF), left ventricular mass (LVM), right ventricular end-systolic volume (RVESV), right ventricular end-diastolic volume (RVEDV) and right ventricular ejection fraction (RVEF). Subgroup analysis included study quality (high, moderate), disease outcomes (disease, healthy and disease), age group (50 years old and under, over 50 years), imaging plane (biplane, multiplane) and publication year (2010 and earlier, after 2010) to determine whether they explained the heterogeneity and significant difference results generated on RT3DE compared to CMR.
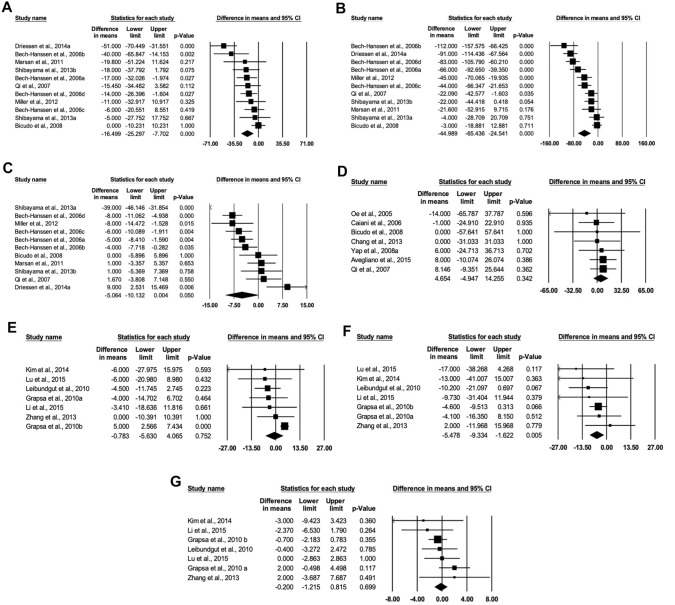
Results: The pooled mean differences for were - 5.064 (95% CI - 10.132, 0.004, p > 0.05), 4.654 (95% CI - 4.947, 14.255, p > 0.05), - 0.783 (95% CI - 5.630, 4.065, p > 0.05, - 0.200 (95% CI - 1.215, 0.815, p > 0.05) for LVEF, LVM, RVESV and RVEF, respectively. We found no significant difference between RT3DE and CMR for these variables. Although, there was a significant difference between RT3DE and CMR for LVESV, LVEDV and RVEDV where RT3DE reports a lower value. Subgroup analysis indicated a significant difference between RT3DE and CMR for studies with participants with an average age of over 50 years but no significant difference for those under 50. In addition, a significant difference between RT3DE and CMR was found in studies using only participants with cardiovascular diseases but not in those using a combination of diseased and healthy participants. Furthermore, for the variables LVESV and LVEDV, the multiplane method shows no significant difference between RT3DE and CMR, as opposed to the biplane showing a significant difference. This potentially indicates that increased age, the presence of cardiovascular disease and the biplane analysis method decrease its concordance with CMR.
Conclusion: This meta-analysis indicates promising results for the use of RT3DE, with limited difference to CMR. Although in some cases, RT3DE appears to underestimate volume, ejection fraction and mass when compared to CMR. Further research is required in terms of imaging method and technology to validate RT3DE for routine clinical use.
Keywords: Cardiac magnetic resonance (CMR); Echocardiography; Left ventricular ejection fraction; Left ventricular end-diastolic volume (LVEDV); Left ventricular end-systolic volume (LVESV); Left ventricular mass (LVM); Right ventricular ejection fraction; Right ventricular end-diastolic volume (RVEDV); Right ventricular end-systolic volume (RVESV).
© 2023. The Author(s).
Conflict of interest statement
There is no conflict of interests for this study.
Figures
References
-
- Sanz JA, Galar M, Jurio A, Brugos A, Pagola M, Bustince H. Medical diagnosis of cardiovascular diseases using an interval-valued fuzzy rule-based classification system. Appl Soft Comput. 2014;20:103–111. doi: 10.1016/j.asoc.2013.11.009. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
