

A convolutional neural network with self-attention for fully automated metabolic tumor volume delineation of head and neck cancer in F]FDG PET/CT
- PMID: 37079128
- PMCID: PMC10317885
- DOI: 10.1007/s00259-023-06197-1
A convolutional neural network with self-attention for fully automated metabolic tumor volume delineation of head and neck cancer in F]FDG PET/CT
Abstract
Purpose: PET-derived metabolic tumor volume (MTV) and total lesion glycolysis of the primary tumor are known to be prognostic of clinical outcome in head and neck cancer (HNC). Including evaluation of lymph node metastases can further increase the prognostic value of PET but accurate manual delineation and classification of all lesions is time-consuming and prone to interobserver variability. Our goal, therefore, was development and evaluation of an automated tool for MTV delineation/classification of primary tumor and lymph node metastases in PET/CT investigations of HNC patients.
Methods: Automated lesion delineation was performed with a residual 3D U-Net convolutional neural network (CNN) incorporating a multi-head self-attention block. 698 F]FDG PET/CT scans from 3 different sites and 5 public databases were used for network training and testing. An external dataset of 181 F]FDG PET/CT scans from 2 additional sites was employed to assess the generalizability of the network. In these data, primary tumor and lymph node (LN) metastases were interactively delineated and labeled by two experienced physicians. Performance of the trained network models was assessed by 5-fold cross-validation in the main dataset and by pooling results from the 5 developed models in the external dataset. The Dice similarity coefficient (DSC) for individual delineation tasks and the primary tumor/metastasis classification accuracy were used as evaluation metrics. Additionally, a survival analysis using univariate Cox regression was performed comparing achieved group separation for manual and automated delineation, respectively.
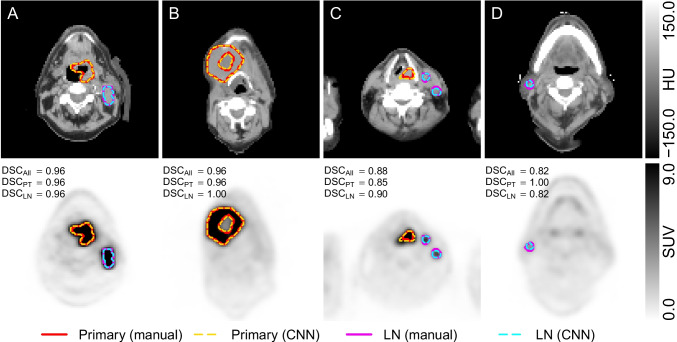
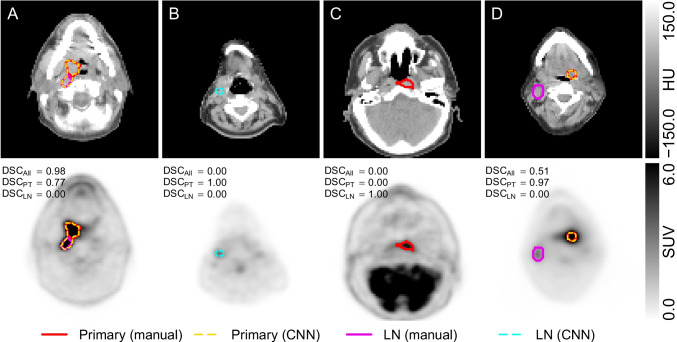
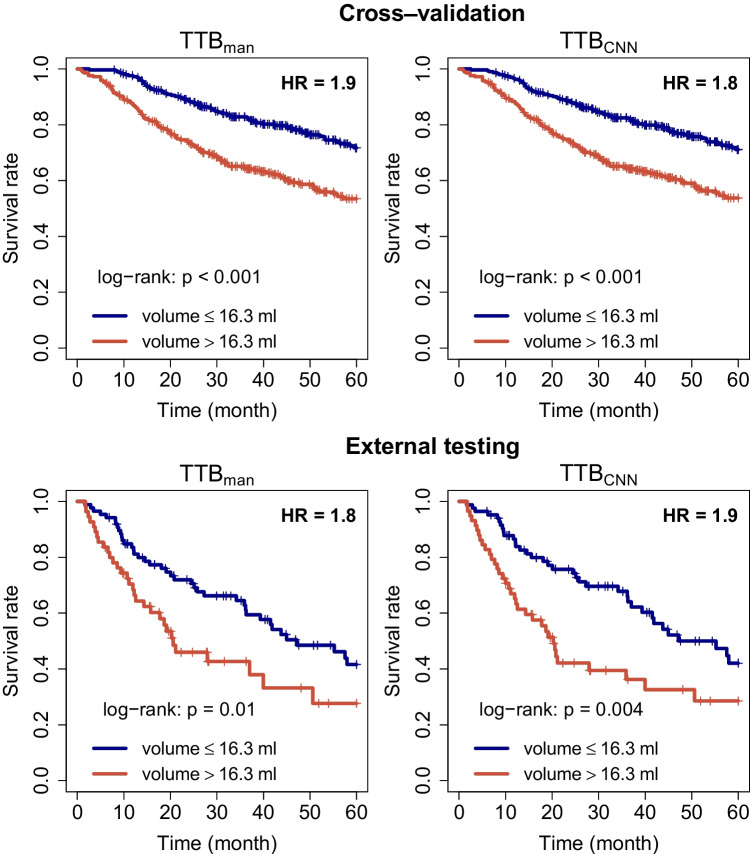
Results: In the cross-validation experiment, delineation of all malignant lesions with the trained U-Net models achieves DSC of 0.885, 0.805, and 0.870 for primary tumor, LN metastases, and the union of both, respectively. In external testing, the DSC reaches 0.850, 0.724, and 0.823 for primary tumor, LN metastases, and the union of both, respectively. The voxel classification accuracy was 98.0% and 97.9% in cross-validation and external data, respectively. Univariate Cox analysis in the cross-validation and the external testing reveals that manually and automatically derived total MTVs are both highly prognostic with respect to overall survival, yielding essentially identical hazard ratios (HR) (; vs. ; in cross-validation and ; vs. ; in external testing).
Conclusion: To the best of our knowledge, this work presents the first CNN model for successful MTV delineation and lesion classification in HNC. In the vast majority of patients, the network performs satisfactory delineation and classification of primary tumor and lymph node metastases and only rarely requires more than minimal manual correction. It is thus able to massively facilitate study data evaluation in large patient groups and also does have clear potential for supervised clinical application.
Keywords: Convolutional neural network; FDG PET; HNC; Head and neck cancer; MTV; Metabolic tumor volume.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Benefits of automated gross tumor volume segmentation in head and neck cancer using multi-modality information.Radiother Oncol. 2023 May;182:109574. doi: 10.1016/j.radonc.2023.109574. Epub 2023 Feb 21. Radiother Oncol. 2023. PMID: 36822358
-
Deep learning for elective neck delineation: More consistent and time efficient.Radiother Oncol. 2020 Dec;153:180-188. doi: 10.1016/j.radonc.2020.10.007. Epub 2020 Oct 14. Radiother Oncol. 2020. PMID: 33065182
-
Prognostic value of metabolic tumor burden on 18F-FDG PET in nonsurgical patients with non-small cell lung cancer.Eur J Nucl Med Mol Imaging. 2012 Jan;39(1):27-38. doi: 10.1007/s00259-011-1934-6. Epub 2011 Sep 23. Eur J Nucl Med Mol Imaging. 2012. PMID: 21946983
-
Diagnostic accuracy of F-18 FDG PET or PET/CT for detection of lymph node metastasis in clinically node negative head and neck cancer patients; A systematic review and meta-analysis.Am J Otolaryngol. 2019 Mar-Apr;40(2):297-305. doi: 10.1016/j.amjoto.2018.10.013. Epub 2018 Oct 23. Am J Otolaryngol. 2019. PMID: 30473166
-
Evaluation of the Prognostic Value of FDG PET/CT Parameters for Patients With Surgically Treated Head and Neck Cancer: A Systematic Review.JAMA Otolaryngol Head Neck Surg. 2020 May 1;146(5):471-479. doi: 10.1001/jamaoto.2020.0014. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 32215611
Cited by
-
Tumor Asphericity in FDG PET Is an Independent Prognostic Parameter Improving Risk Stratification in Patients with Head and Neck Squamous Cell Carcinoma.J Nucl Med. 2025 May 1;66(5):686-691. doi: 10.2967/jnumed.124.268972. J Nucl Med. 2025. PMID: 40081960
-
Total lesion glycolysis of primary tumor and lymphnodes is a strong predictor for development of distant metastases in oropharyngeal carcinoma patients with independent validation in automatically delineated lesions.Cancer Imaging. 2025 Feb 21;25(1):18. doi: 10.1186/s40644-025-00836-6. Cancer Imaging. 2025. PMID: 39985091 Free PMC article.
References
-
- Nichols AC, Theurer J, Prisman E, Read N, Berthelet E, Tran E, et al. Radiotherapy versus transoral robotic surgery and neck dissection for oropharyngeal squamous cell carcinoma (ORATOR): an open-label, phase 2, randomised trial. Lancet Oncol. 2019;20(10):1349–59. doi: 10.1016/S1470-2045(19)30410-3. - DOI - PubMed
-
- Zschaeck S, Li Y, Lin Q, Beck M, Amthauer H, Bauersachs L, et al. Prognostic value of baseline [18F]-fluorodeoxyglucose positron emission tomography parameters MTV, TLG and asphericity in an international multicenter cohort of nasopharyngeal carcinoma patients. PLoS ONE. 2020;15(7):e0236841. doi: 10.1371/journal.pone.0236841. - DOI - PMC - PubMed
-
- Zschaeck S, Weingärtner J, Lombardo E, Marschner S, Hajiyianni M, Beck M, et al. 18F-Fluorodeoxyglucose positron emission tomography of head and neck cancer: location and HPV specific parameters for potential treatment individualization. Front Oncol. 2022;12. 10.3389/fonc.2022.870319. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
