

Early Detection of Molecular Residual Disease and Risk Stratification for Stage I to III Colorectal Cancer via Circulating Tumor DNA Methylation
- PMID: 37079312
- PMCID: PMC10119774
- DOI: 10.1001/jamaoncol.2023.0425
Early Detection of Molecular Residual Disease and Risk Stratification for Stage I to III Colorectal Cancer via Circulating Tumor DNA Methylation
Abstract
Importance: Detection of molecular residual disease and risk stratification as early as possible may improve the treatment of patients with cancer. Efficient pragmatic tests are therefore required.
Objective: To measure circulating tumor DNA (ctDNA) with 6 DNA methylation markers in blood samples and to evaluate the association of the presence of ctDNA with colorectal cancer (CRC) recurrence throughout the disease course.
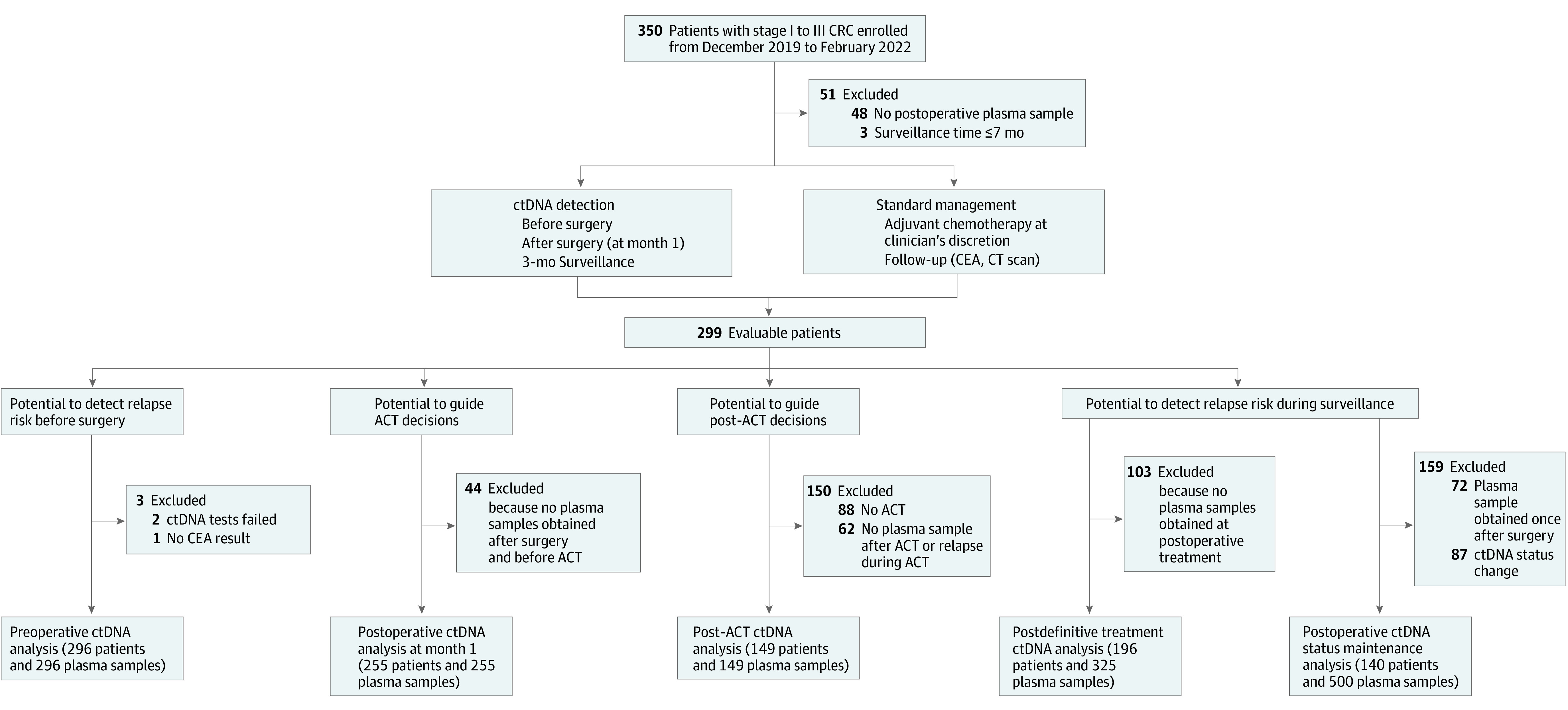
Design, setting, and participants: In this multicenter prospective longitudinal cohort study performed from December 12, 2019, to February 28, 2022, 350 patients with stage I to III CRC were recruited from 2 hospitals for collection of blood samples before and after surgery, during and after adjuvant chemotherapy, and every 3 months for up to 2 years. A multiplex, ctDNA methylation, quantitative polymerase chain reaction assay was used to detect ctDNA in plasma samples.
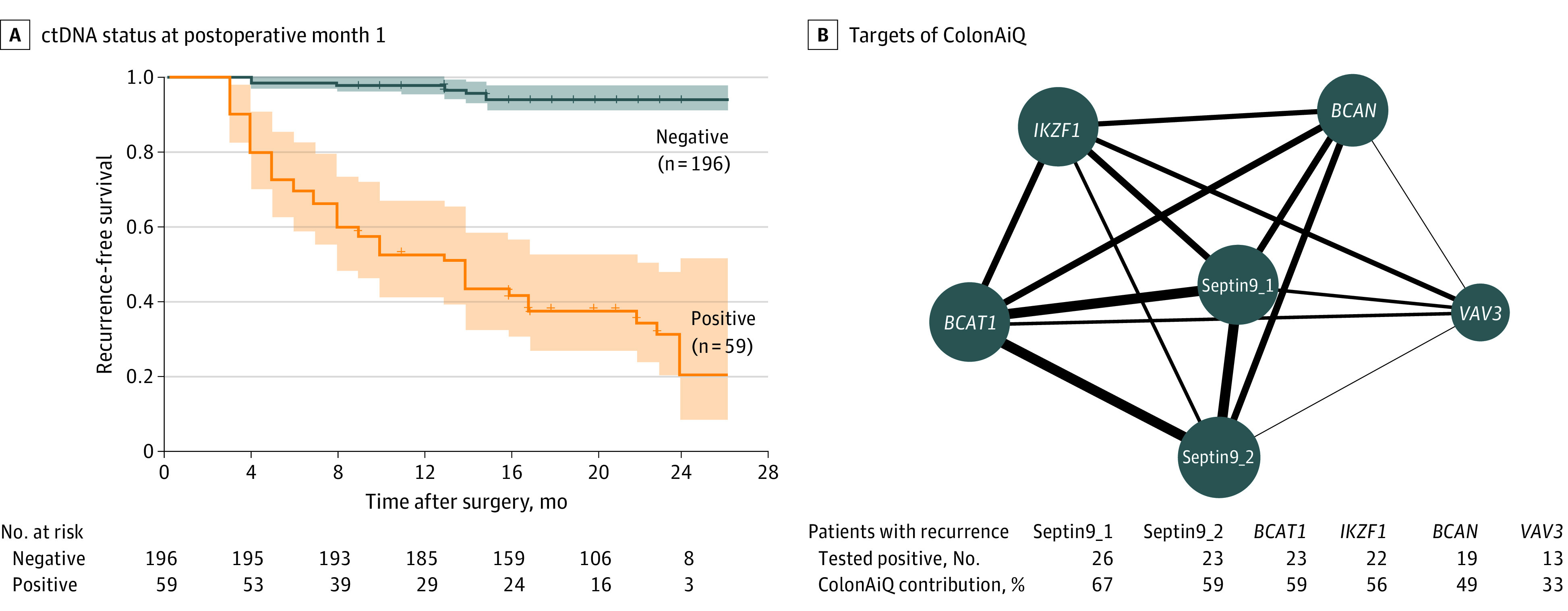
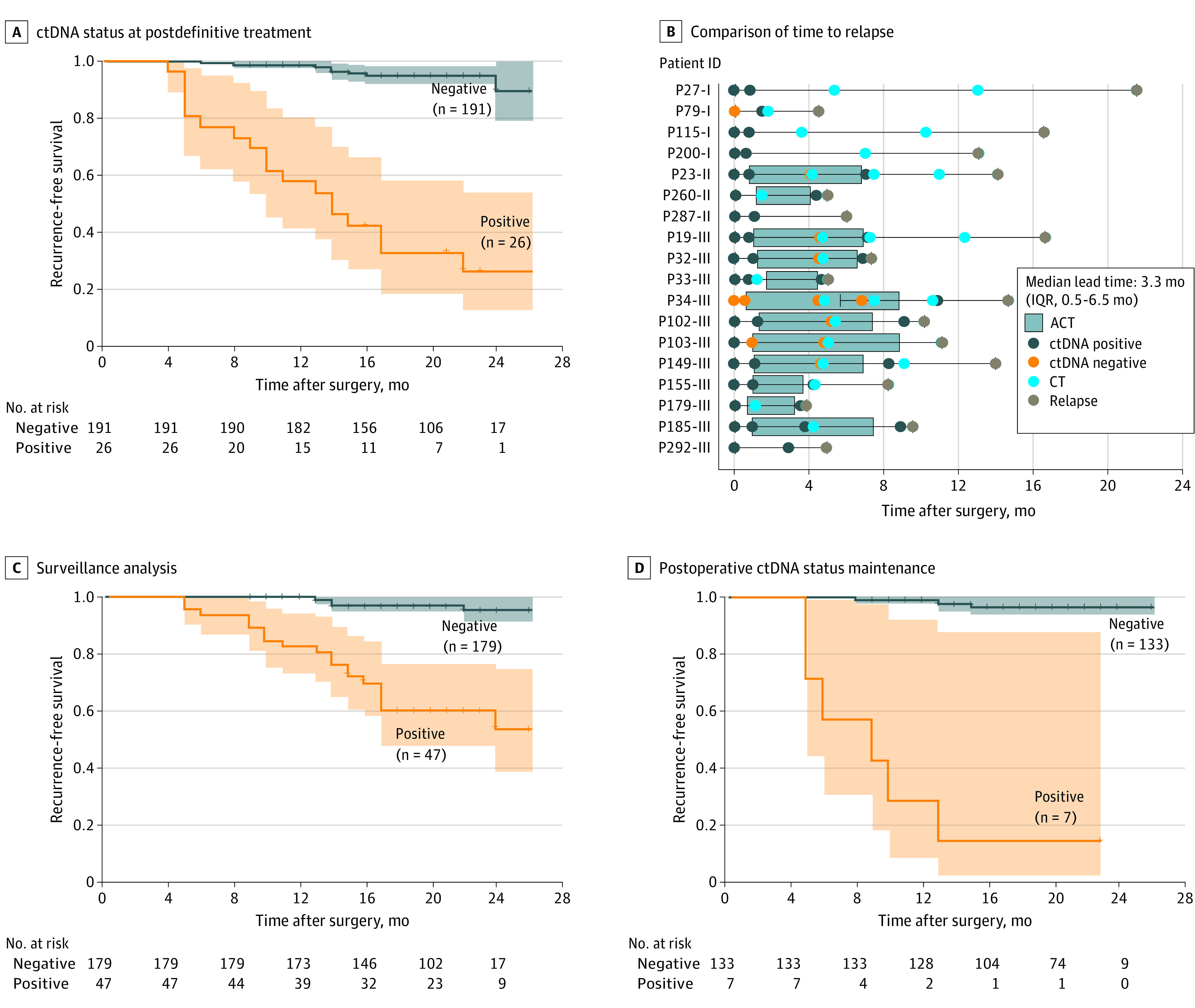
Results: A total of 299 patients with stage I to III CRC were evaluated. Of 296 patients with preoperative samples, 232 (78.4%) tested positive for any of the 6 ctDNA methylation markers. A total of 186 patients (62.2%) were male, and the mean (SD) age was 60.1 (10.3) years. At postoperative month 1, ctDNA-positive patients were 17.5 times more likely to relapse than were ctDNA-negative patients (hazard ratio [HR], 17.5; 95% CI, 8.9-34.4; P < .001). The integration of ctDNA and carcinoembryonic antigen tests showed risk stratification for recurrence with an HR of 19.0 (95% CI, 8.9-40.7; P < .001). Furthermore, ctDNA status at postoperative month 1 was strongly associated with prognosis in patients treated with adjuvant chemotherapy of different durations and intensities. After adjuvant chemotherapy, ctDNA-positive patients had a significantly shorter recurrence-free survival than did the ctDNA-negative patients (HR, 13.8; 95% CI, 5.9-32.1; P < .001). Longitudinal ctDNA analysis after the postdefinitive treatment showed a discriminating effect in that ctDNA-positive patients had poorer recurrence-free survival than did the ctDNA-negative patients (HR, 20.6; 95% CI, 9.5-44.9; P < .001). The discriminating effect was enhanced (HR, 68.8; 95% CI, 18.4-257.7; P < .001) when ctDNA status was maintained longitudinally. Postdefinitive treatment analysis detected CRC recurrence earlier than radiologically confirmed recurrence, with a median lead time of 3.3 months (IQR, 0.5-6.5 months).
Conclusions and relevance: The findings of this cohort study suggest that longitudinal assessment of ctDNA methylation may enable the early detection of recurrence, potentially optimizing risk stratification and postoperative treatment of patients with CRC.
Conflict of interest statement
Figures
Comment in
-
Liquid Biopsy Assessment of Molecular Residual Disease in Localized Colorectal Cancer: Is It Ready for Prime Time?JAMA Oncol. 2023 Jun 1;9(6):763-764. doi: 10.1001/jamaoncol.2023.0329. JAMA Oncol. 2023. PMID: 37079293 No abstract available.
Similar articles
-
Tissue-Free Liquid Biopsies Combining Genomic and Methylation Signals for Minimal Residual Disease Detection in Patients with Early Colorectal Cancer from the UK TRACC Part B Study.Clin Cancer Res. 2024 Aug 15;30(16):3459-3469. doi: 10.1158/1078-0432.CCR-24-0226. Clin Cancer Res. 2024. PMID: 38864835 Free PMC article.
-
Circulating tumor DNA is a prognostic marker of tumor recurrence in stage II and III colorectal cancer: multicentric, prospective cohort study (ALGECOLS).Eur J Cancer. 2021 Dec;159:24-33. doi: 10.1016/j.ejca.2021.09.004. Epub 2021 Oct 30. Eur J Cancer. 2021. PMID: 34731746
-
Postoperative circulating tumor DNA as markers of recurrence risk in stages II to III colorectal cancer.J Hematol Oncol. 2021 May 17;14(1):80. doi: 10.1186/s13045-021-01089-z. J Hematol Oncol. 2021. PMID: 34001194 Free PMC article.
-
Circulating Tumor DNA as a Real-Time Biomarker for Minimal Residual Disease and Recurrence Prediction in Stage II Colorectal Cancer: A Systematic Review and Meta-Analysis.Int J Mol Sci. 2025 Mar 11;26(6):2486. doi: 10.3390/ijms26062486. Int J Mol Sci. 2025. PMID: 40141130 Free PMC article.
-
Circulating tumor DNA as a prognostic indicator of colorectal cancer recurrence-a systematic review and meta-analysis.Int J Colorectal Dis. 2022 May;37(5):1021-1027. doi: 10.1007/s00384-022-04144-4. Epub 2022 Apr 6. Int J Colorectal Dis. 2022. PMID: 35384496 Free PMC article.
Cited by
-
Decoding the Dynamics of Circulating Tumor DNA in Liquid Biopsies.Cancers (Basel). 2024 Jul 1;16(13):2432. doi: 10.3390/cancers16132432. Cancers (Basel). 2024. PMID: 39001494 Free PMC article. Review.
-
Colorectal cancer screening using a multi-locus blood-based assay targeting circulating tumor DNA methylation: a cross-sectional study in an average-risk population.BMC Med. 2024 Nov 27;22(1):560. doi: 10.1186/s12916-024-03777-2. BMC Med. 2024. PMID: 39604913 Free PMC article.
-
Circulating Tumor DNA in the Monitoring of Soft Tissue Sarcoma Treatment and Recurrence.Ann Surg Oncol. 2024 Nov;31(12):7682-7684. doi: 10.1245/s10434-024-15902-9. Epub 2024 Jul 26. Ann Surg Oncol. 2024. PMID: 39060690 No abstract available.
-
Development and validation of cancer-specific survival prediction nomogram for patients with T4 stage colon cancer after surgical resection: a population-based study.Int J Colorectal Dis. 2025 Mar 18;40(1):72. doi: 10.1007/s00384-025-04856-3. Int J Colorectal Dis. 2025. PMID: 40102264 Free PMC article.
-
Dissecting cell-free DNA fragmentation variation in tumors using cell line-derived xenograft mouse.PLoS One. 2025 Jul 15;20(7):e0327483. doi: 10.1371/journal.pone.0327483. eCollection 2025. PLoS One. 2025. PMID: 40663513 Free PMC article.
