

Ageing, functioning patterns and their environmental determinants in the spinal cord injury (SCI) population: A comparative analysis across eleven European countries implementing the International Spinal Cord Injury Community Survey
- PMID: 37079622
- PMCID: PMC10118153
- DOI: 10.1371/journal.pone.0284420
Ageing, functioning patterns and their environmental determinants in the spinal cord injury (SCI) population: A comparative analysis across eleven European countries implementing the International Spinal Cord Injury Community Survey
Abstract
Background: As the European population with Spinal Cord Injury (SCI) is expected to become older, a better understanding of ageing with SCI using functioning, the health indicator used to model healthy ageing trajectories, is needed. We aimed to describe patterns of functioning in SCI by chronological age, age at injury and time since injury across eleven European countries using a common functioning metric, and to identify country-specific environmental determinants of functioning.
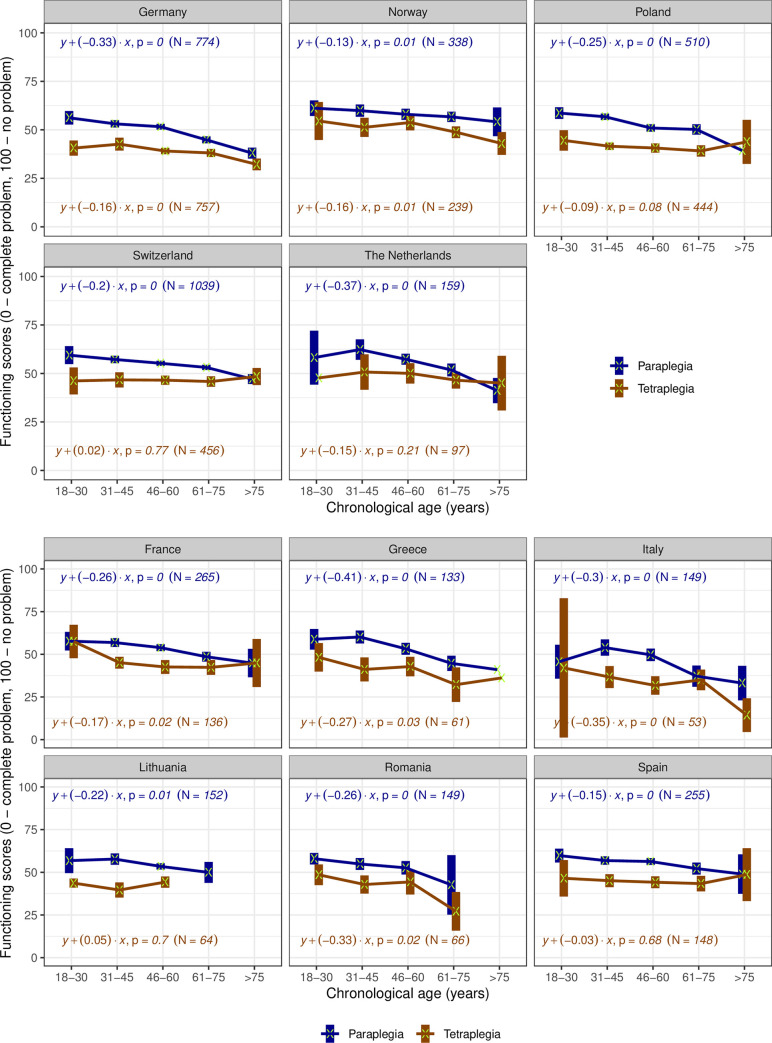
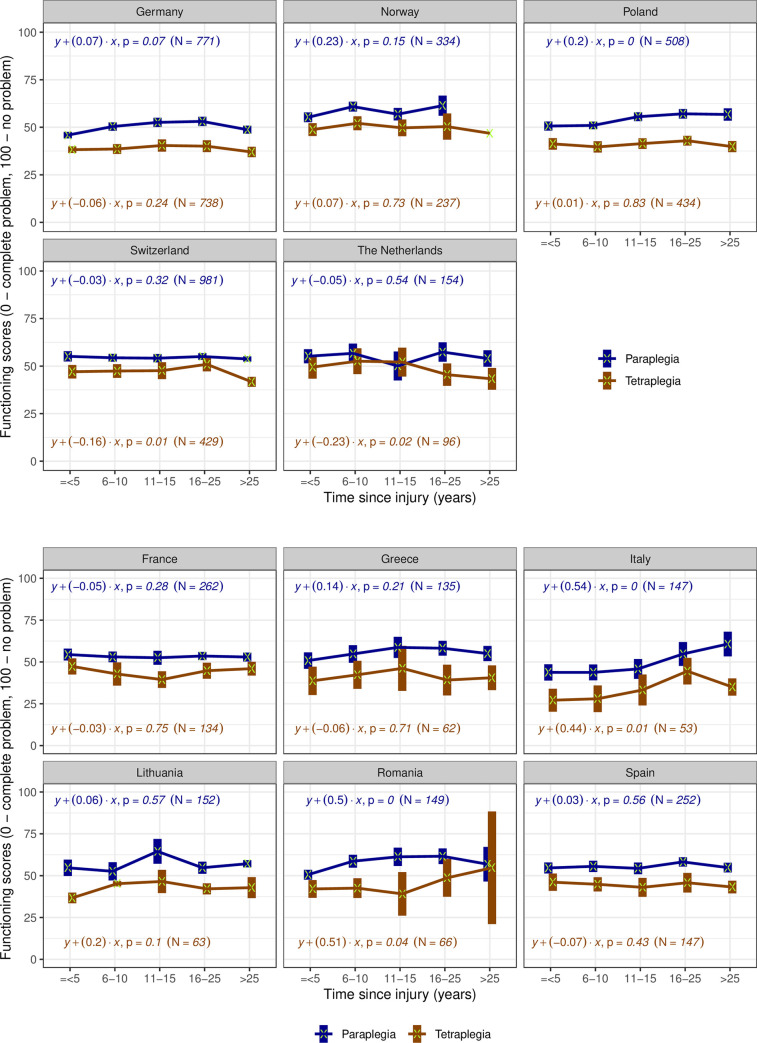
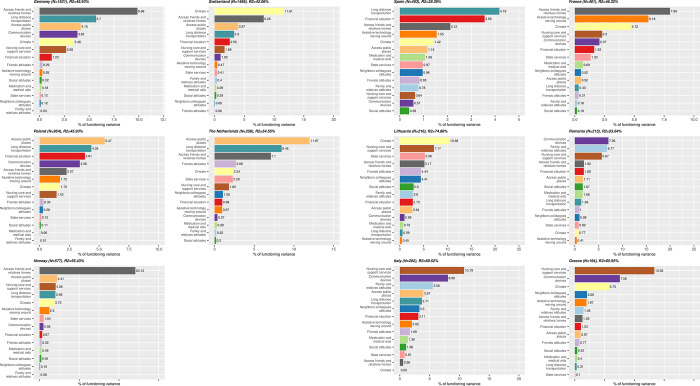
Methods: Data from 6'635 participants of the International Spinal Cord Injury Community Survey was used. The hierarchical version of Generalized Partial Credit Model, casted in a Bayesian framework, was used to create a common functioning metric and overall scores. For each country, linear regression was used to investigate associations between functioning, chronological age, age at SCI or time since injury for persons with para- and tetraplegia. Multiple linear regression and the proportional marginal variance decomposition technique were used to identify environmental determinants.
Results: In countries with representative samples older chronological age was consistently associated with a decline in functioning for paraplegia but not for tetraplegia. Age at injury and functioning level were associated, but patterns differed across countries. An association between time since injury and functioning was not observed in most countries, neither for paraplegia nor for tetraplegia. Problems with the accessibility of homes of friends and relatives, access to public places and long-distance transportation were consistently key determinants of functioning.
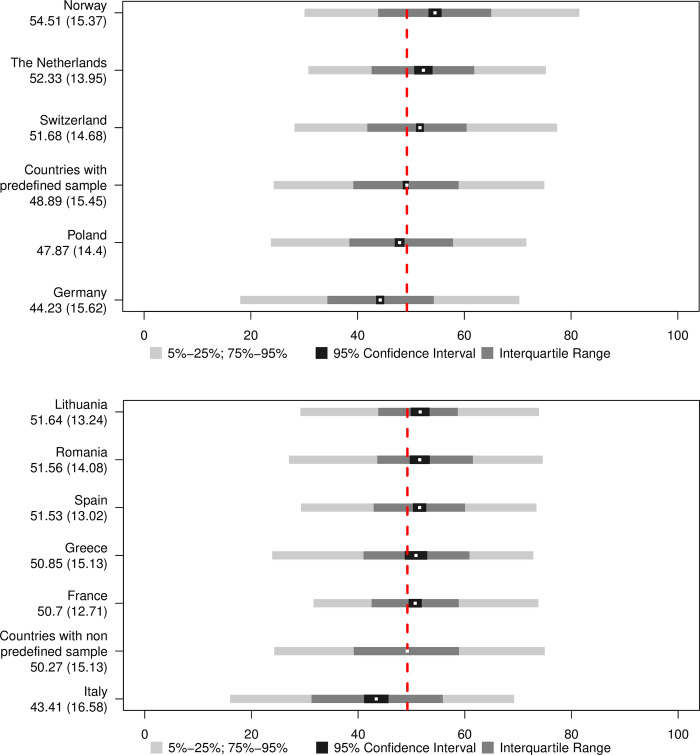
Conclusions: Functioning is a key health indicator and the fundament of ageing research. Enhancing methods traditionally used to develop metrics with Bayesian approach, we were able to create a common metric of functioning with cardinal properties and to estimate overall scores comparable across countries. Focusing on functioning, our study complements epidemiological evidence on SCI-specific mortality and morbidity in Europe and identify initial targets for evidence-informed policy-making.
Copyright: © 2023 Sabariego et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Grassner L, Marschallinger J, Dunser MW, Novak HF, Zerbs A, Aigner L, et al. Nontraumatic spinal cord injury at the neurological intensive care unit: spectrum, causes of admission and predictors of mortality. Ther Adv Neurol Disord. 2016;9[2]:85–94. doi: 10.1177/1756285615621687 - DOI - PMC - PubMed
-
- Bickenbach JE, Biering-Sorensen F, Knott J, Shakespeare T, Stucki G, Tharion G. Understanding spinal cord injury. International perspectives on spinal cord injury. Geneva: WHO; 2013. p. 3–10.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
