

Sustained release hydrogel for durable locoregional chemoimmunotherapy for BRAF-mutated melanoma
- PMID: 37080489
- PMCID: PMC10328138
- DOI: 10.1016/j.jconrel.2023.04.028
Sustained release hydrogel for durable locoregional chemoimmunotherapy for BRAF-mutated melanoma
Erratum in
-
Corrigendum to "Sustained release hydrogel for durable locoregional chemoimmunotherapy for BRAF-mutated melanoma" [Journal of Controlled Release 357 (2023) 655-668].J Control Release. 2024 Feb;366:834-837. doi: 10.1016/j.jconrel.2023.11.055. Epub 2024 Jan 29. J Control Release. 2024. PMID: 38290359 Free PMC article. No abstract available.
Abstract
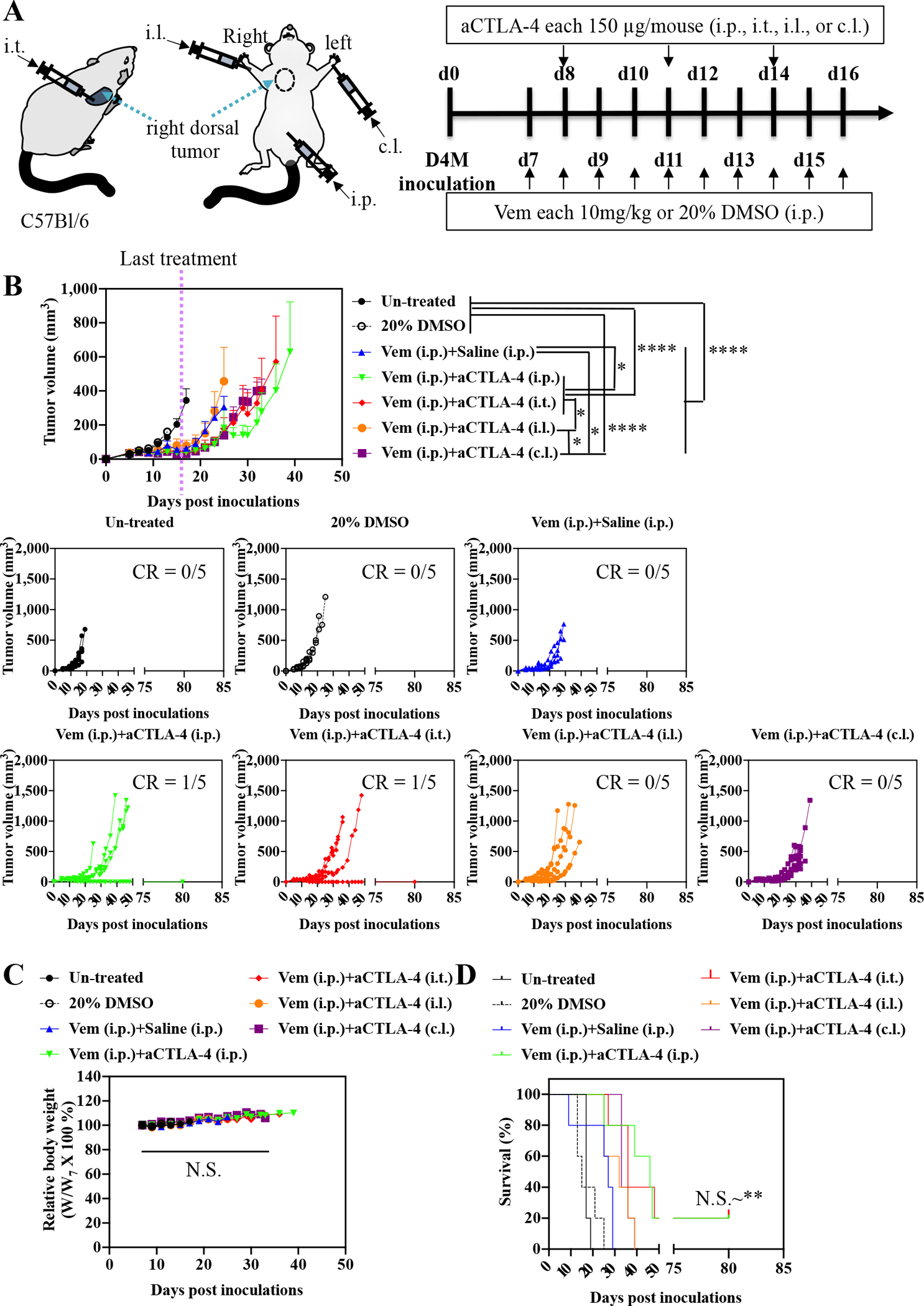
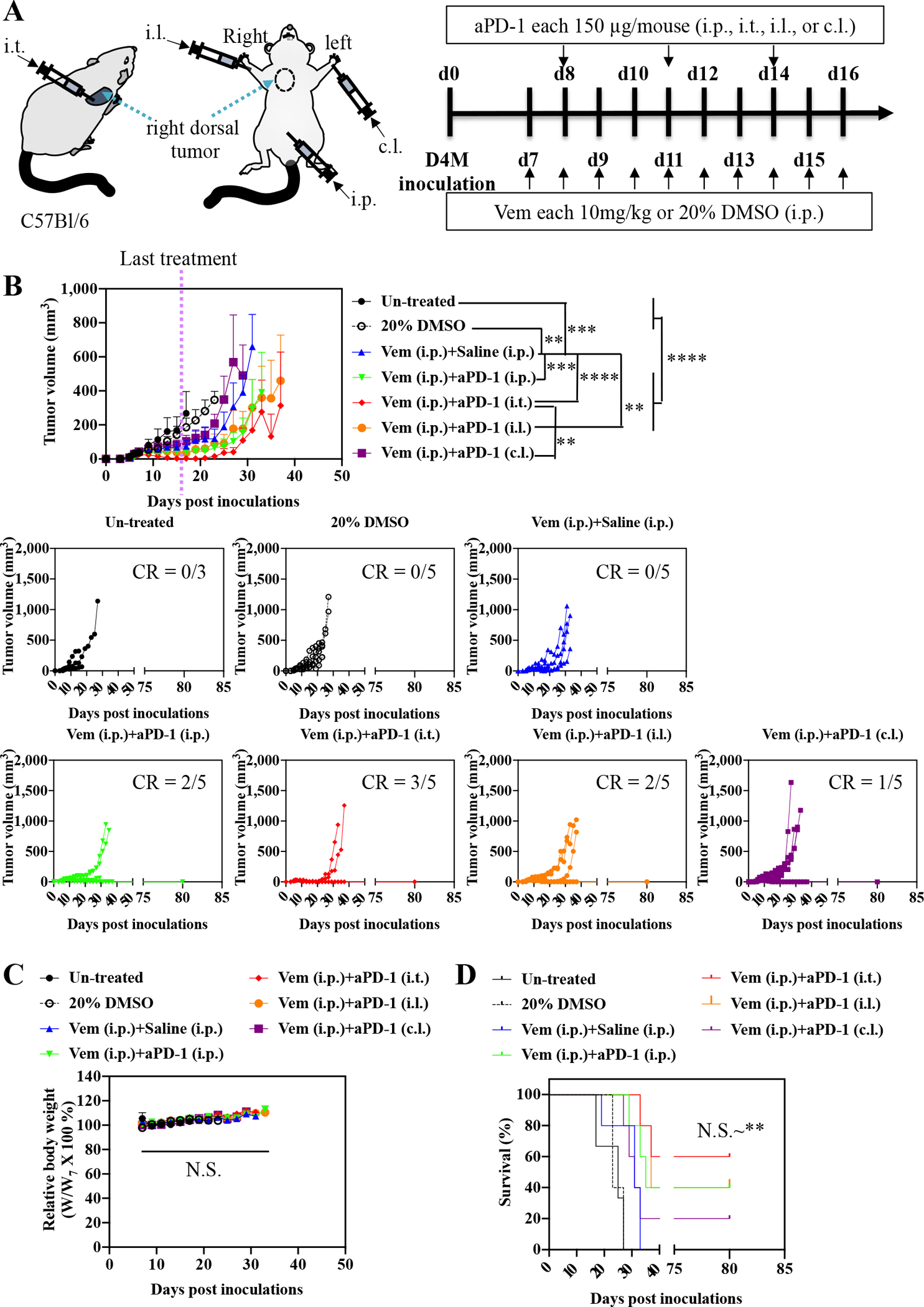
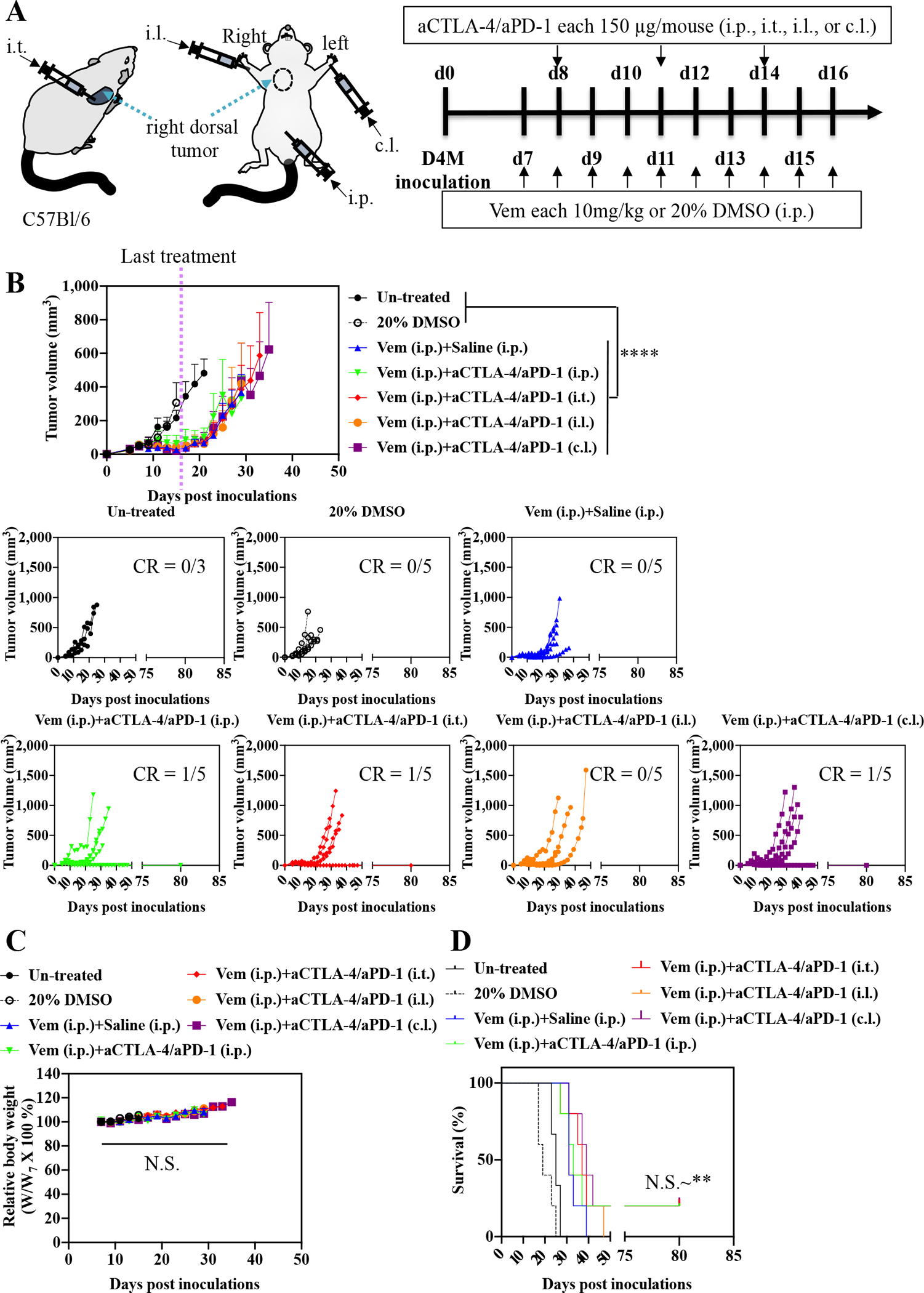
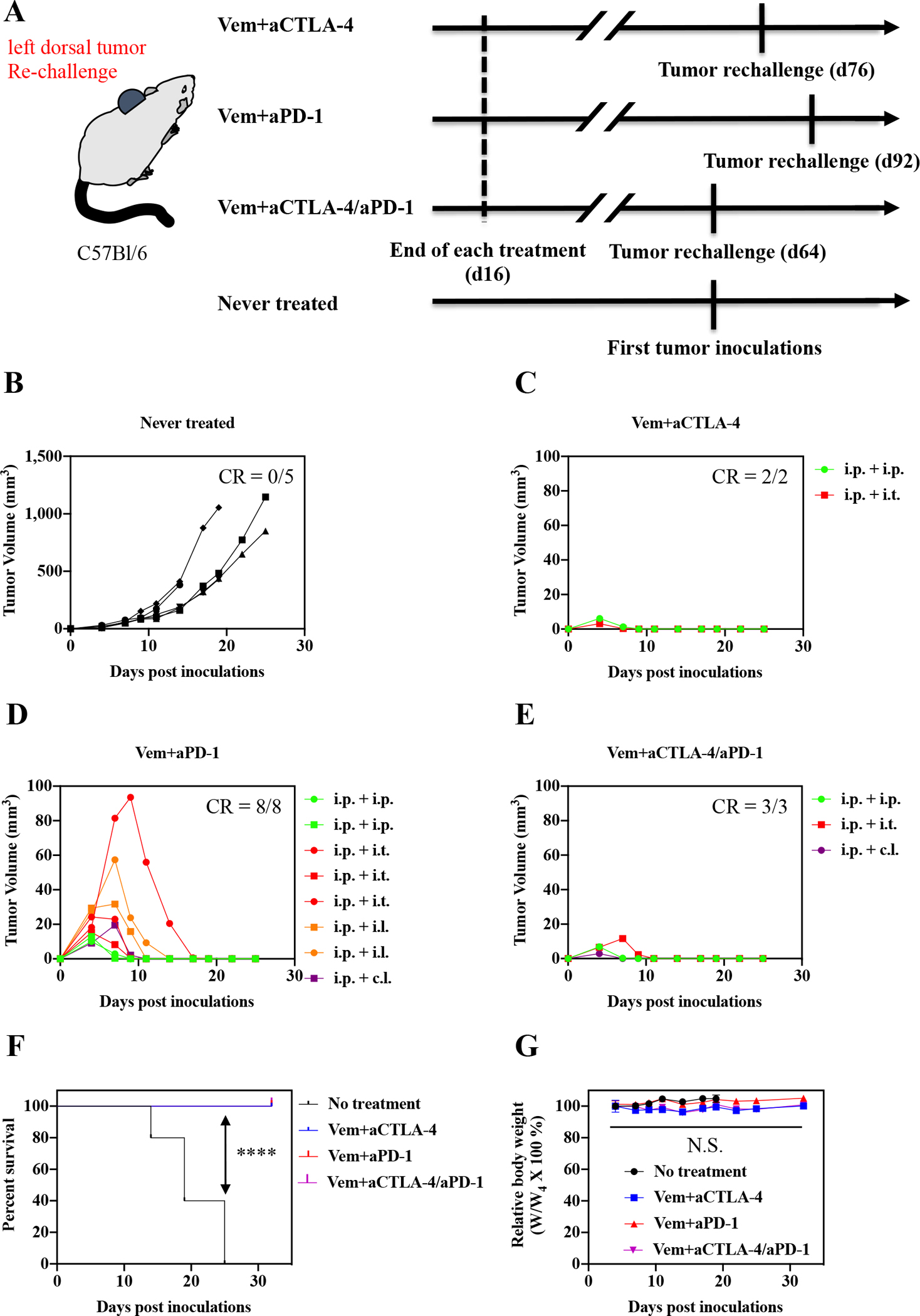
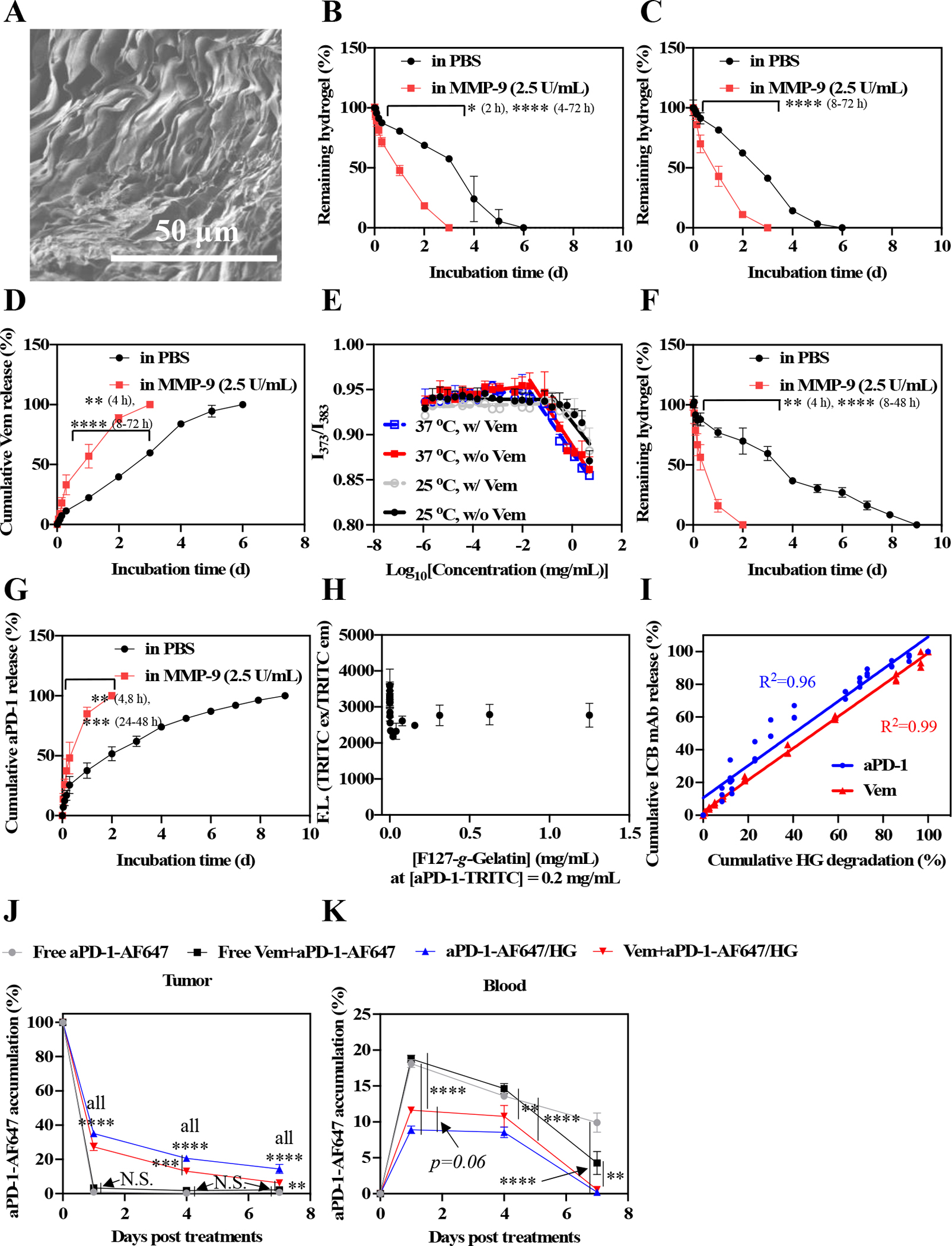
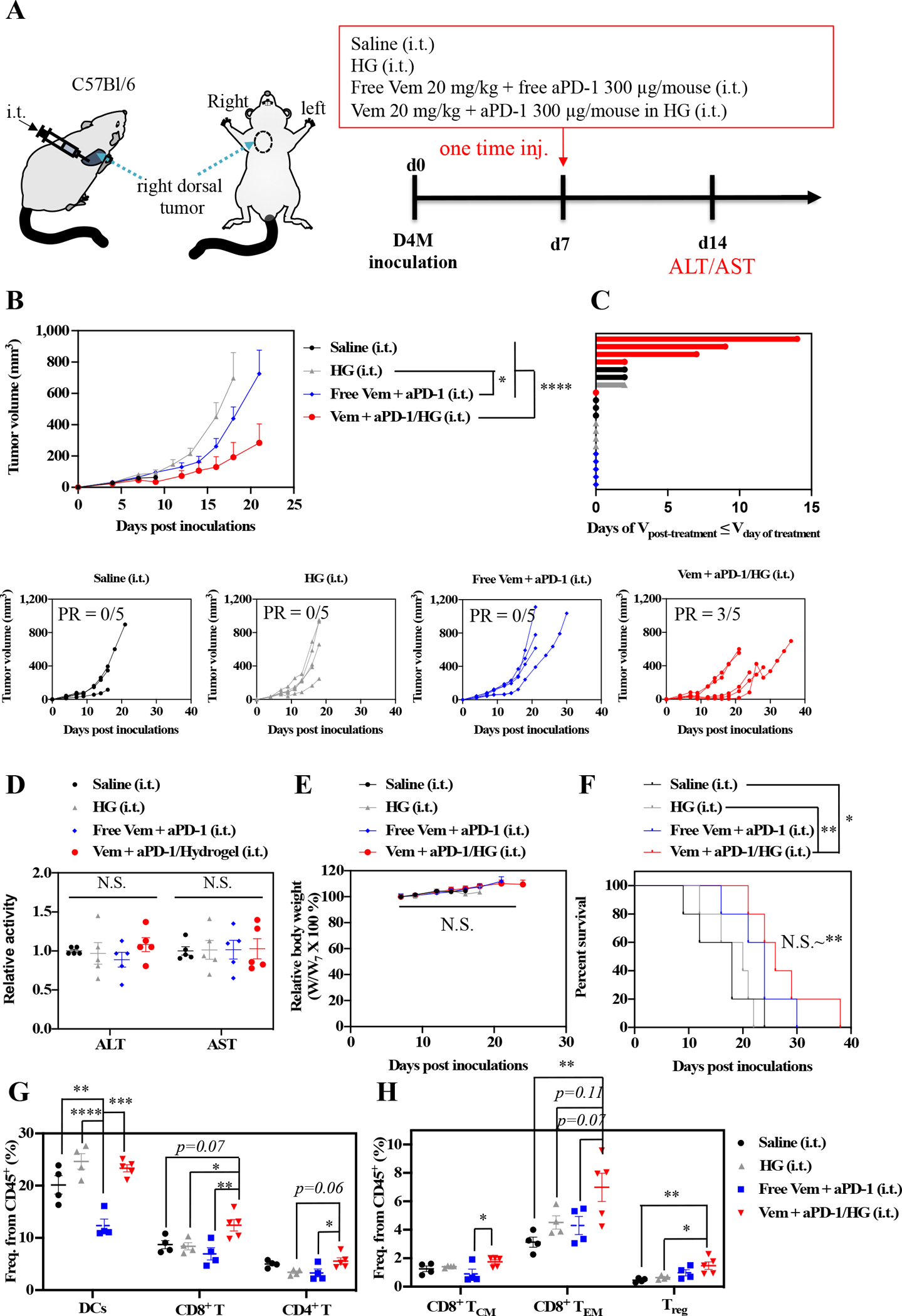
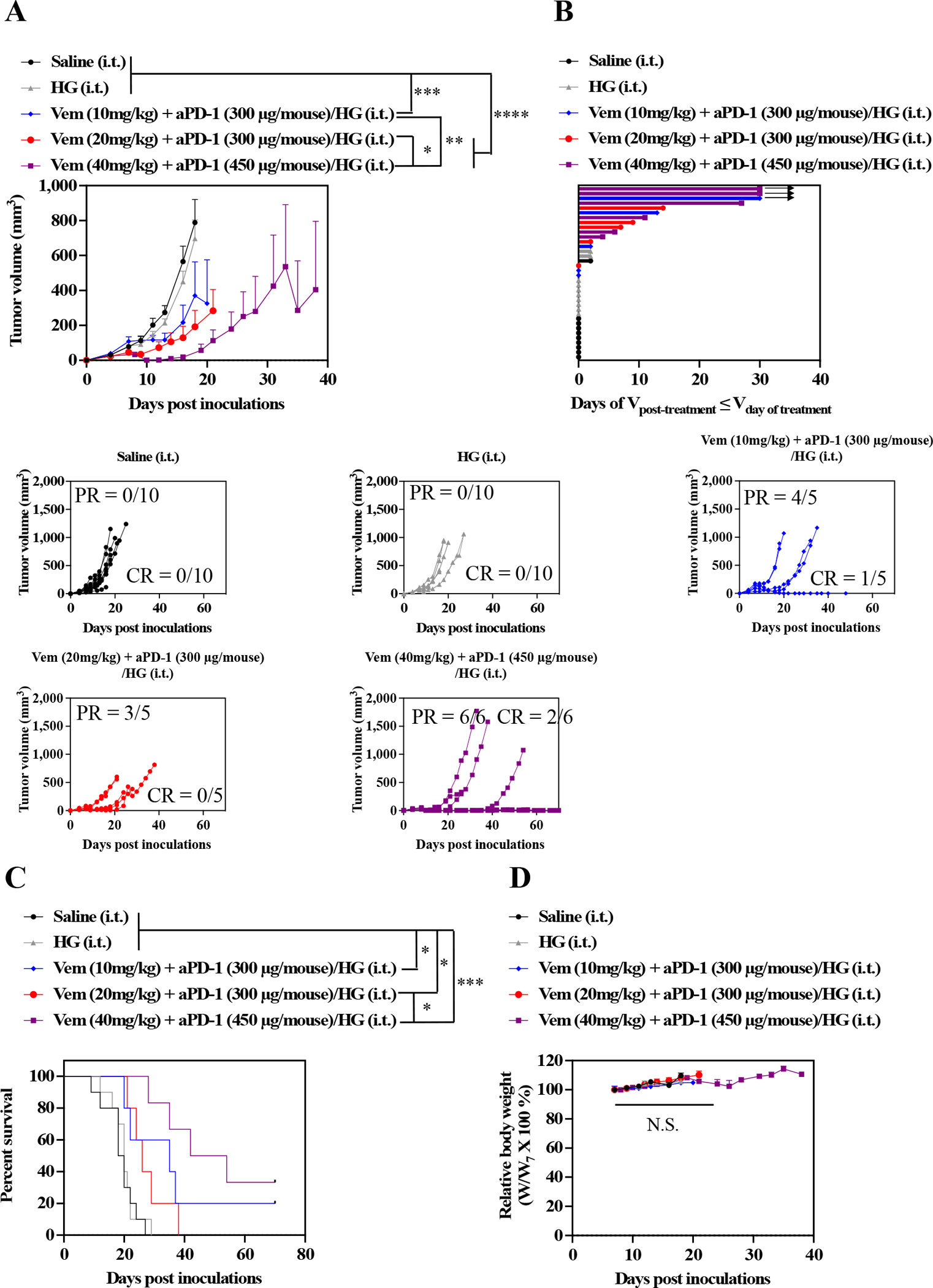
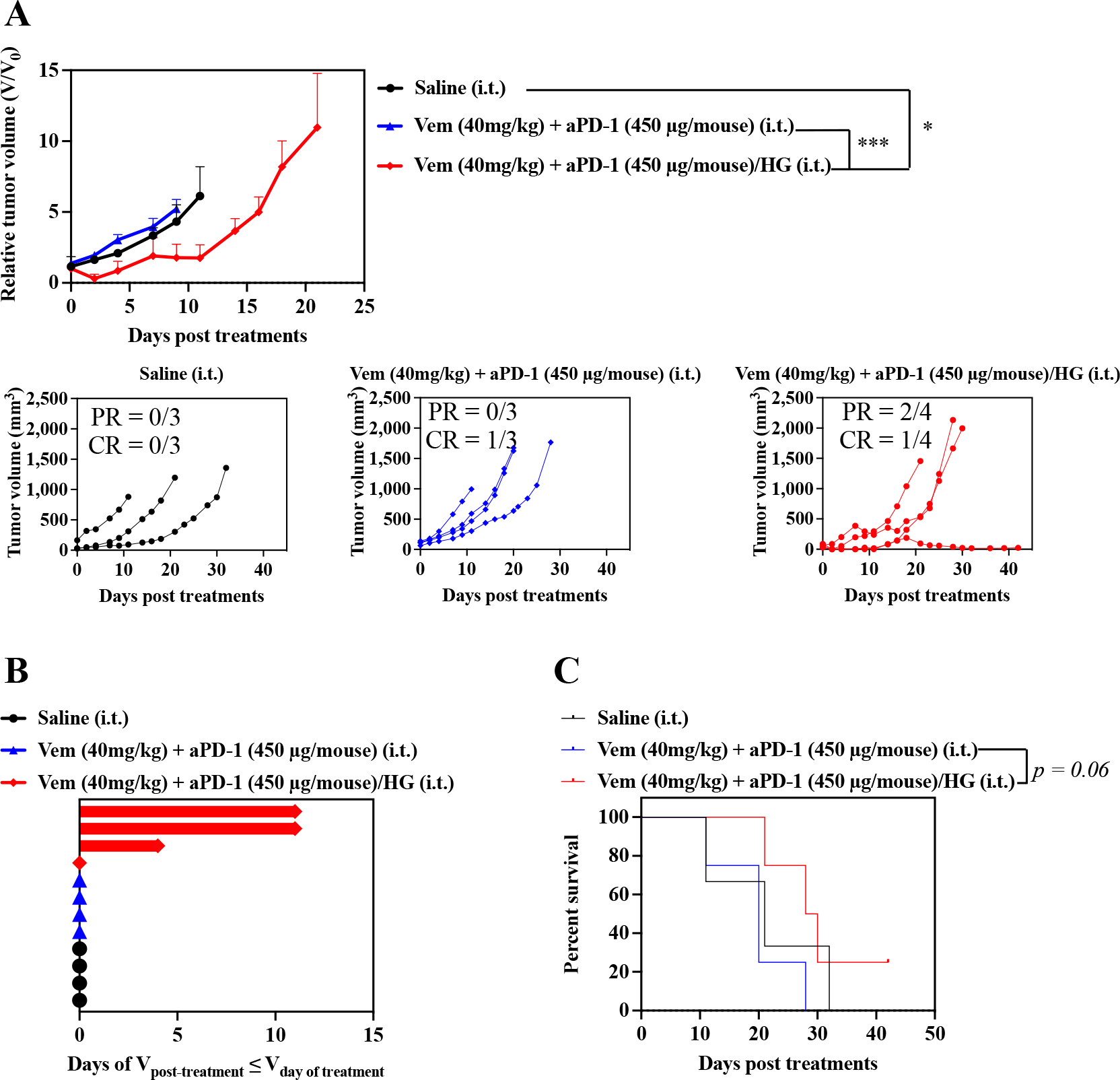
The wide prevalence of BRAF mutations in diagnosed melanomas drove the clinical advancement of BRAF inhibitors in combination with immune checkpoint blockade for treatment of advanced disease. However, deficits in therapeutic potencies and safety profiles motivate the development of more effective strategies that improve the combination therapy's therapeutic index. Herein, we demonstrate the benefits of a locoregional chemoimmunotherapy delivery system, a novel thermosensitive hydrogel comprised of gelatin and Pluronic® F127 components already widely used in humans in both commercial and clinical products, for the co-delivery of a small molecule BRAF inhibitor with immune checkpoint blockade antibody for the treatment of BRAF-mutated melanoma. In vivo evaluation of administration route and immune checkpoint target effects revealed intratumoral administration of antagonistic programmed cell death protein 1 antibody (aPD-1) lead to potent antitumor therapy in combination with BRAF inhibitor vemurafenib. The thermosensitive F127-g-Gelatin hydrogel that was evaluated in multiple murine models of BRAF-mutated melanoma that facilitated prolonged local drug release within the tumor (>1 week) substantially improved local immunomodulation, tumor control, rates of tumor response, and animal survival. Thermosensitive F127-g-Gelatin hydrogels thus improve upon the clinical benefits of vemurafenib and aPD-1 in a locoregional chemoimmunotherapy approach for the treatment of BRAF-mutated melanoma.
Keywords: BRAF inhibitor; Drug delivery system; Immune checkpoint blockade; Sustained release; Thermosensitive hydrogel.
Copyright © 2023. Published by Elsevier B.V.
Conflict of interest statement
Declaration of competing interest J.K. and S.N.T. are inventors on a submitted patent related to the technology described in this manuscript.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
