

Clinical decision support with a comprehensive in-EHR patient tracking system improves genetic testing follow up
- PMID: 37080563
- PMCID: PMC10280356
- DOI: 10.1093/jamia/ocad070
Clinical decision support with a comprehensive in-EHR patient tracking system improves genetic testing follow up
Abstract
Objective: We sought to develop and evaluate an electronic health record (EHR) genetic testing tracking system to address the barriers and limitations of existing spreadsheet-based workarounds.
Materials and methods: We evaluated the spreadsheet-based system using mixed effects logistic regression to identify factors associated with delayed follow up. These factors informed the design of an EHR-integrated genetic testing tracking system. After deployment, we assessed the system in 2 ways. We analyzed EHR access logs and note data to assess patient outcomes and performed semistructured interviews with users to identify impact of the system on work.
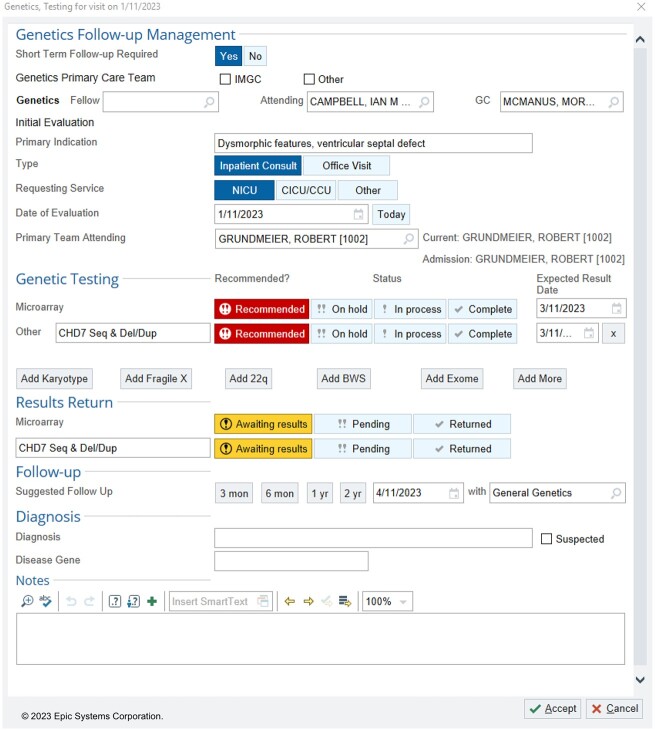
Results: We found that patient-reported race was a significant predictor of documented genetic testing follow up, indicating a possible inequity in care. We implemented a CDS system including a patient data capture form and management dashboard to facilitate important care tasks. The system significantly sped review of results and significantly increased documentation of follow-up recommendations. Interviews with key system users identified a range of sociotechnical factors (ie, tools, tasks, collaboration) that contribute to safer and more efficient care.
Discussion: Our new tracking system ended decades of workarounds for identifying and communicating test results and improved clinical workflows. Interview participants related that the system decreased cognitive and time burden which allowed them to focus on direct patient interaction.
Conclusion: By assembling a multidisciplinary team, we designed a novel patient tracking system that improves genetic testing follow up. Similar approaches may be effective in other clinical settings.
Keywords: clinical decision support; genetic testing; transition of care.
© The Author(s) 2023. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
The authors have no competing interests.
Figures





References
-
- Ross LF, Saal HM, David KL, et al.; American College of Medical Genetics and Genomics and the American Academy of Pediatrics. Technical report: ethical and policy issues in genetic testing and screening of children. Genet Med 2013; 15 (3): 234–45. - PubMed
-
- Scott A, Martin DM.. Development and implementation of an electronic medical record module to track genetic testing results. Genet Med 2021; 23 (5): 972–5. - PubMed
-
- Poon EG, Gandhi TK, Sequist TD, et al.“I wish i had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med 2004; 164 (20): 2223–8. - PubMed
