

Hypnotic prescription trends and patterns for the treatment of insomnia in Japan: analysis of a nationwide Japanese claims database
- PMID: 37081408
- PMCID: PMC10120113
- DOI: 10.1186/s12888-023-04683-2
Hypnotic prescription trends and patterns for the treatment of insomnia in Japan: analysis of a nationwide Japanese claims database
Abstract
Background: There is limited consensus regarding the optimal treatment of insomnia. The recent introduction of orexin receptor antagonists (ORA) has increased the available treatment options. However, the prescribing patterns of hypnotics in Japan have not been comprehensively assessed. We performed analyses of a claims database to investigate the real-world use of hypnotics for treating insomnia in Japan.
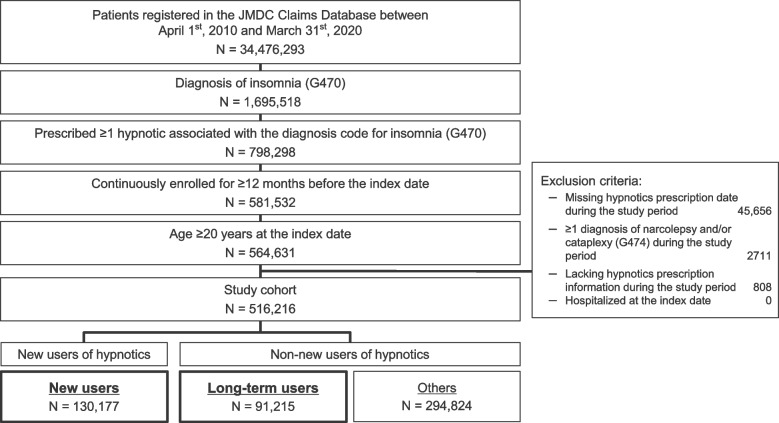
Methods: Data were retrieved for outpatients (aged ≥ 20 to < 75 years old) prescribed ≥ 1 hypnotic for a diagnosis of insomnia between April 1st, 2009 and March 31st, 2020, with ≥ 12 months of continuous enrolment in the JMDC Claims Database. Patients were classified as new or long-term users of hypnotics. Long-term use was defined as prescription of the same mechanism of action (MOA) for ≥ 180 days. We analyzed the trends (2010-2019) and patterns (2018-2019) in hypnotics prescriptions.
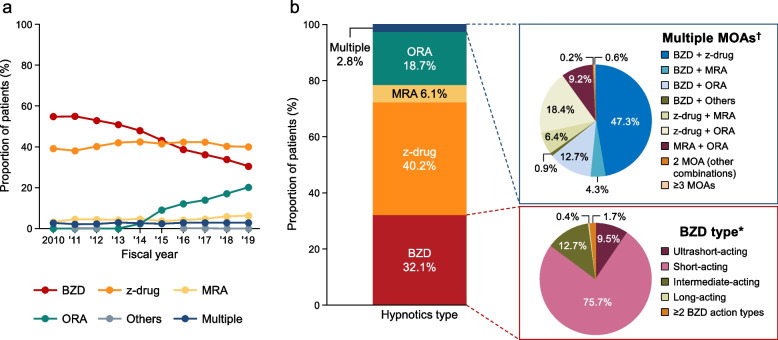
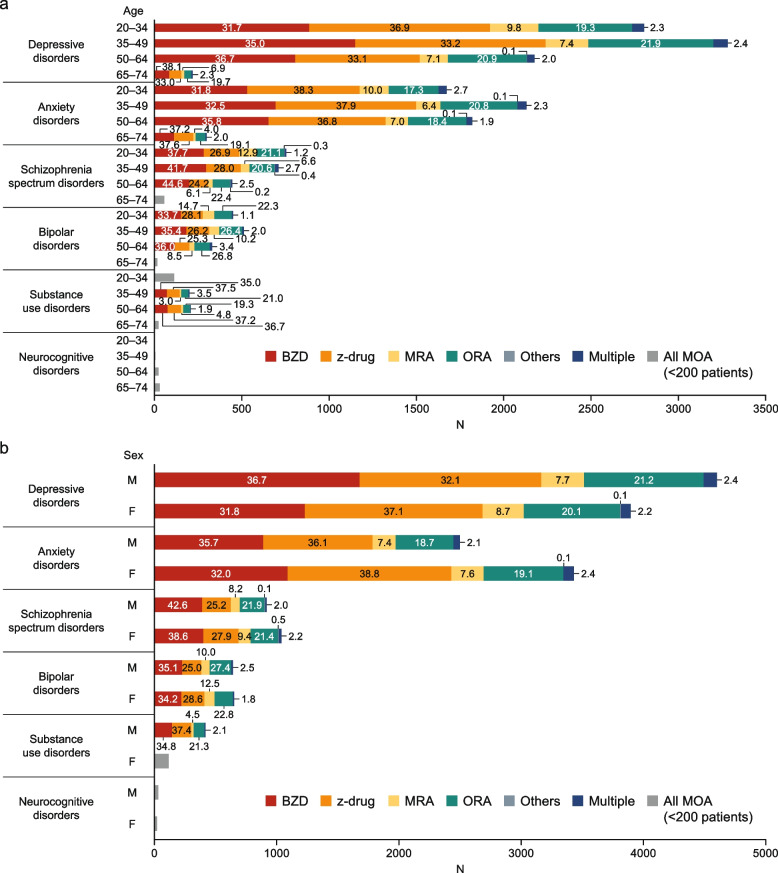
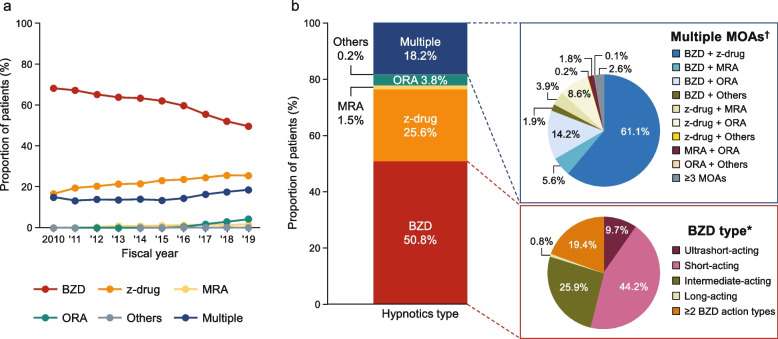
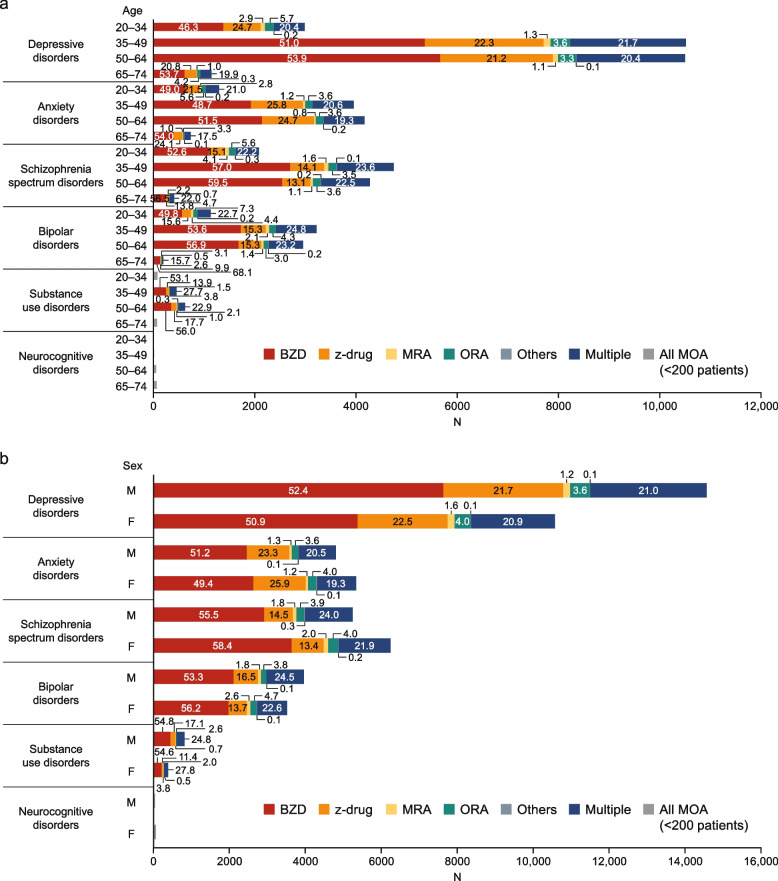
Results: We analyzed data for 130,177 new and 91,215 long-term users (2010-2019). Most new users were prescribed one MOA per year (97.1%-97.9%). In 2010, GABAA-receptor agonists (benzodiazepines [BZD] or z-drugs) were prescribed to 94.0% of new users. Prescriptions for BZD declined from 54.8% of patients in 2010 to 30.5% in 2019, whereas z-drug prescriptions remained stable (~ 40%). Prescriptions for melatonin receptor agonist increased slightly (3.2% to 6.3%). Prescriptions for ORA increased over this time from 0% to 20.2%. Prescriptions for BZD alone among long-term users decreased steadily from 68.3% in 2010 to 49.7% in 2019. Prescriptions for ORA were lower among long-term users (0% in 2010, 4.3% in 2019) relative to new users. Using data from 2018-2019, multiple (≥ 2) MOAs were prescribed to a higher proportion of long-term (18.2%) than new (2.8%) users. The distribution of MOAs according to psychiatric comorbidities, segmented by age or sex, revealed higher proportions of BZD prescriptions in elderly (new and long-term users) and male (new users) patients in all comorbidity segments.
Conclusion: Prescriptions for hypnotics among new and long-term users in Japan showed distinct patterns and trends. Further understanding of the treatment options for insomnia with accumulating evidence for the risk-benefit balance might be beneficial for physicians prescribing hypnotics in real-world settings.
Keywords: Benzodiazepine; Claims database; Hypnotics; Insomnia; Japan; Melatonin receptor antagonist; Orexin receptor antagonist; Prescriptions; z-drugs.
© 2023. Merck & Co., Inc., Rahway, NJ, USA and its affiliates.
Conflict of interest statement
SO, YY, and ST are employees of MSD K.K., Tokyo, Japan, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and may own stock and/or hold stock options in Merck & Co., Inc., Rahway, NJ, USA. ZPQ was an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and may have owned stock and/or stock options in Merck & Co., Inc., Rahway, NJ, USA at the time of the study. YH is an employee of JMDC Inc. and CI was an employee of JMDC Inc. at the time of the study.
Figures
Similar articles
-
Trends in prescriptions for sedative-hypnotics among Korean adults: a nationwide prescription database study for 2011-2015.Soc Psychiatry Psychiatr Epidemiol. 2019 Apr;54(4):477-484. doi: 10.1007/s00127-018-1615-x. Epub 2018 Nov 7. Soc Psychiatry Psychiatr Epidemiol. 2019. PMID: 30406284
-
Effects of Japanese policies and novel hypnotics on long-term prescriptions of hypnotics.Psychiatry Clin Neurosci. 2023 May;77(5):264-272. doi: 10.1111/pcn.13525. Epub 2023 Jan 26. Psychiatry Clin Neurosci. 2023. PMID: 36579672 Free PMC article.
-
Factors Associated with Prescriptions for an Orexin Receptor Antagonist Among Japanese Patients with Insomnia: Analysis of a Nationwide Japanese Claims Database.Drugs Real World Outcomes. 2023 Jun;10(2):271-281. doi: 10.1007/s40801-023-00356-4. Epub 2023 Mar 3. Drugs Real World Outcomes. 2023. PMID: 36867350 Free PMC article.
-
Hypnotic Discontinuation in Chronic Insomnia.Sleep Med Clin. 2022 Sep;17(3):523-530. doi: 10.1016/j.jsmc.2022.06.014. Sleep Med Clin. 2022. PMID: 36150811 Review.
-
Insomnia: Pharmacologic Treatment.Clin Geriatr Med. 2021 Aug;37(3):401-415. doi: 10.1016/j.cger.2021.04.003. Epub 2021 Jun 4. Clin Geriatr Med. 2021. PMID: 34210446 Review.
Cited by
-
Lemborexant-induced interstitial lung disease: A case report.Respirol Case Rep. 2024 Apr 25;12(5):e01334. doi: 10.1002/rcr2.1334. eCollection 2024 May. Respirol Case Rep. 2024. PMID: 38680666 Free PMC article.
-
The effect of education regarding treatment guidelines for schizophrenia and major depressive disorders on psychiatrists' hypnotic medication prescribing behavior: a multicenter study.BMC Psychiatry. 2024 May 29;24(1):399. doi: 10.1186/s12888-024-05816-x. BMC Psychiatry. 2024. PMID: 38807065 Free PMC article.
-
Association between polypharmacy and the long-term prescription of hypnotics in Japan: a retrospective cross-sectional study.Front Psychiatry. 2024 Dec 9;15:1471457. doi: 10.3389/fpsyt.2024.1471457. eCollection 2024. Front Psychiatry. 2024. PMID: 39717375 Free PMC article.
-
Initial treatment choices for long-term remission of chronic insomnia disorder in adults: a systematic review and network meta-analysis.Psychiatry Clin Neurosci. 2024 Nov;78(11):646-653. doi: 10.1111/pcn.13730. Epub 2024 Aug 26. Psychiatry Clin Neurosci. 2024. PMID: 39188094 Free PMC article.
-
Characteristics of psychiatric patients with nightmares after suvorexant administration: A retrospective study.Neuropsychopharmacol Rep. 2025 Mar;45(1):e12506. doi: 10.1002/npr2.12506. Epub 2024 Nov 29. Neuropsychopharmacol Rep. 2025. PMID: 39612917 Free PMC article.
References
-
- Wilson SJ, Nutt DJ, Alford C, Argyropoulos SV, Baldwin DS, Bateson AN, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders. J Psychopharmacol. 2010;24(11):1577–1601. doi: 10.1177/0269881110379307. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
