

Utilization of mechanical power and associations with clinical outcomes in brain injured patients: a secondary analysis of the extubation strategies in neuro-intensive care unit patients and associations with outcome (ENIO) trial
- PMID: 37081474
- PMCID: PMC10120226
- DOI: 10.1186/s13054-023-04410-z
Utilization of mechanical power and associations with clinical outcomes in brain injured patients: a secondary analysis of the extubation strategies in neuro-intensive care unit patients and associations with outcome (ENIO) trial
Abstract
Background: There is insufficient evidence to guide ventilatory targets in acute brain injury (ABI). Recent studies have shown associations between mechanical power (MP) and mortality in critical care populations. We aimed to describe MP in ventilated patients with ABI, and evaluate associations between MP and clinical outcomes.
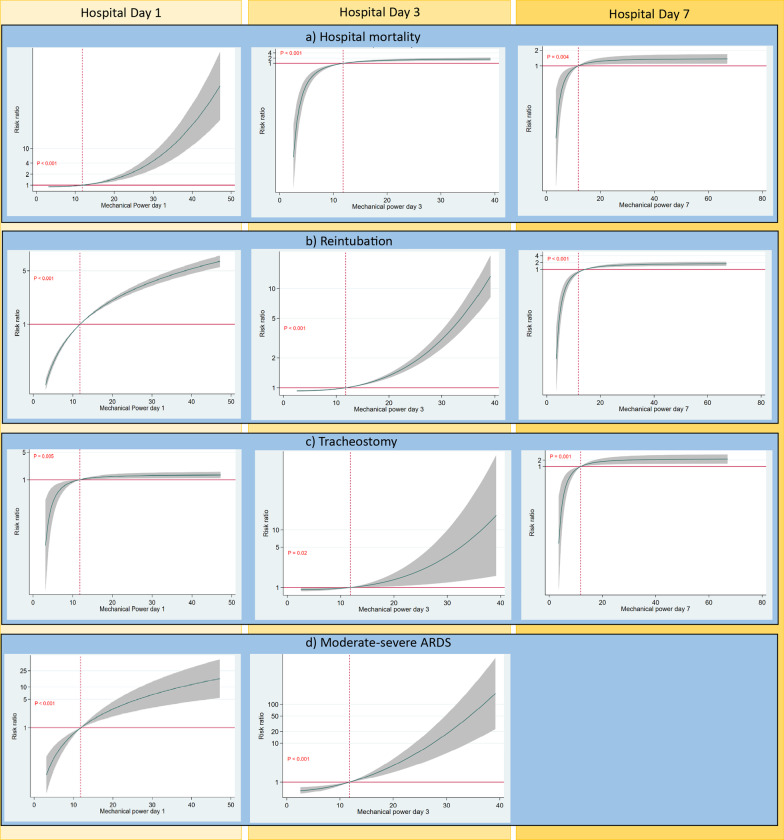
Methods: In this preplanned, secondary analysis of a prospective, multi-center, observational cohort study (ENIO, NCT03400904), we included adult patients with ABI (Glasgow Coma Scale ≤ 12 before intubation) who required mechanical ventilation (MV) ≥ 24 h. Using multivariable log binomial regressions, we separately assessed associations between MP on hospital day (HD)1, HD3, HD7 and clinical outcomes: hospital mortality, need for reintubation, tracheostomy placement, and development of acute respiratory distress syndrome (ARDS).
Results: We included 1217 patients (mean age 51.2 years [SD 18.1], 66% male, mean body mass index [BMI] 26.3 [SD 5.18]) hospitalized at 62 intensive care units in 18 countries. Hospital mortality was 11% (n = 139), 44% (n = 536) were extubated by HD7 of which 20% (107/536) required reintubation, 28% (n = 340) underwent tracheostomy placement, and 9% (n = 114) developed ARDS. The median MP on HD1, HD3, and HD7 was 11.9 J/min [IQR 9.2-15.1], 13 J/min [IQR 10-17], and 14 J/min [IQR 11-20], respectively. MP was overall higher in patients with ARDS, especially those with higher ARDS severity. After controlling for same-day pressure of arterial oxygen/fraction of inspired oxygen (P/F ratio), BMI, and neurological severity, MP at HD1, HD3, and HD7 was independently associated with hospital mortality, reintubation and tracheostomy placement. The adjusted relative risk (aRR) was greater at higher MP, and strongest for: mortality on HD1 (compared to the HD1 median MP 11.9 J/min, aRR at 17 J/min was 1.22, 95% CI 1.14-1.30) and HD3 (1.38, 95% CI 1.23-1.53), reintubation on HD1 (1.64; 95% CI 1.57-1.72), and tracheostomy on HD7 (1.53; 95%CI 1.18-1.99). MP was associated with the development of moderate-severe ARDS on HD1 (2.07; 95% CI 1.56-2.78) and HD3 (1.76; 95% CI 1.41-2.22).
Conclusions: Exposure to high MP during the first week of MV is associated with poor clinical outcomes in ABI, independent of P/F ratio and neurological severity. Potential benefits of optimizing ventilator settings to limit MP warrant further investigation.
Keywords: Acute brain injury; Acute ischemic stroke; Acute respiratory distress syndrome; Intracranial hemorrhage; Mechanical power; Mechanical ventilation; Subarachnoid hemorrhage; Traumatic brain injury.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Robba C, Rebora P, Banzato E, et al. Incidence, risk factors, and effects on outcome of ventilator-associated pneumonia in patients with traumatic brain injury: analysis of a large, multicenter, prospective, observational longitudinal study. Chest. 2020;158(6):2292–2303. doi: 10.1016/j.chest.2020.06.064. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
