

Cholangiocarcinoma Resembling IgG4-related Sclerosing Cholangitis
- PMID: 37081688
- PMCID: PMC10749809
- DOI: 10.2169/internalmedicine.1144-22
Cholangiocarcinoma Resembling IgG4-related Sclerosing Cholangitis
Abstract
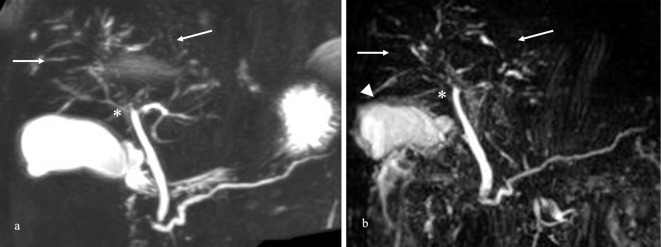
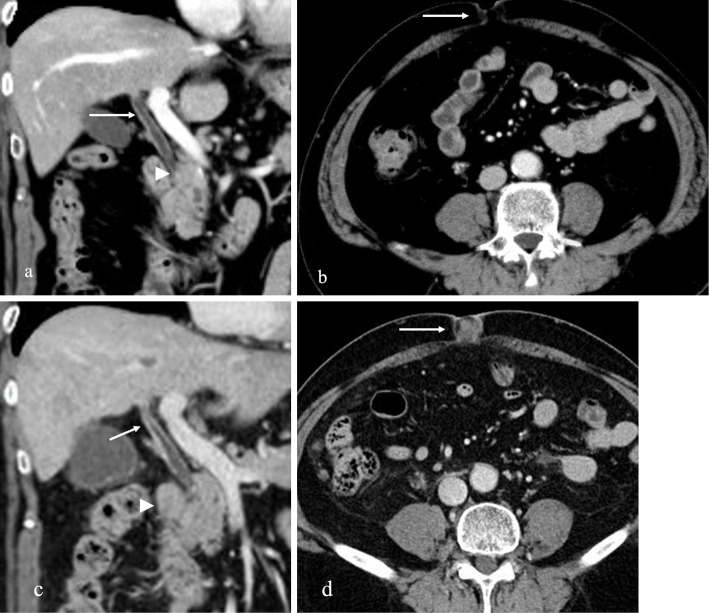
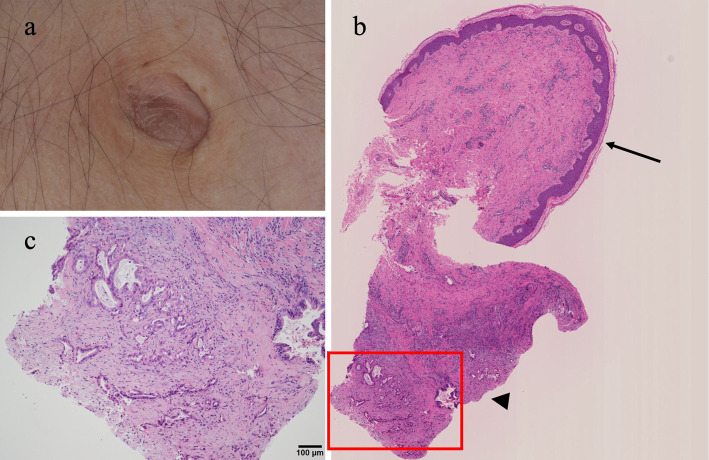
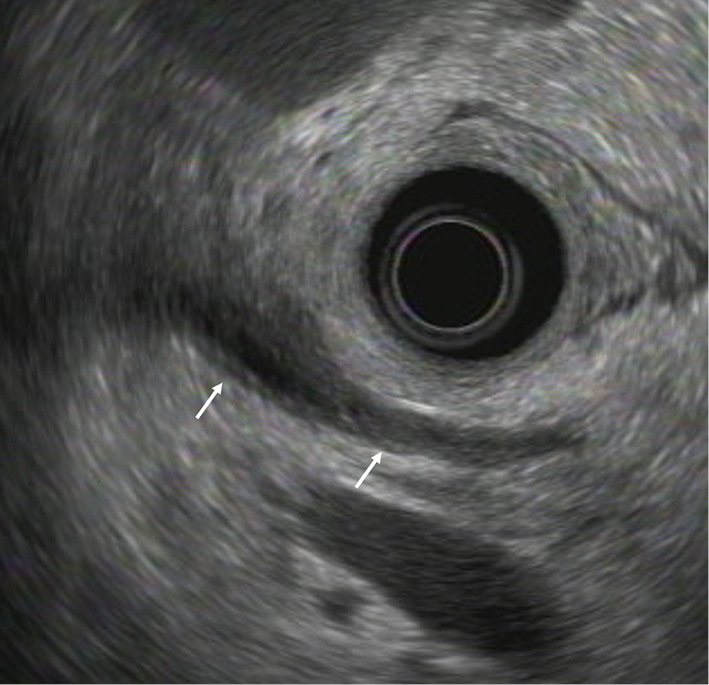
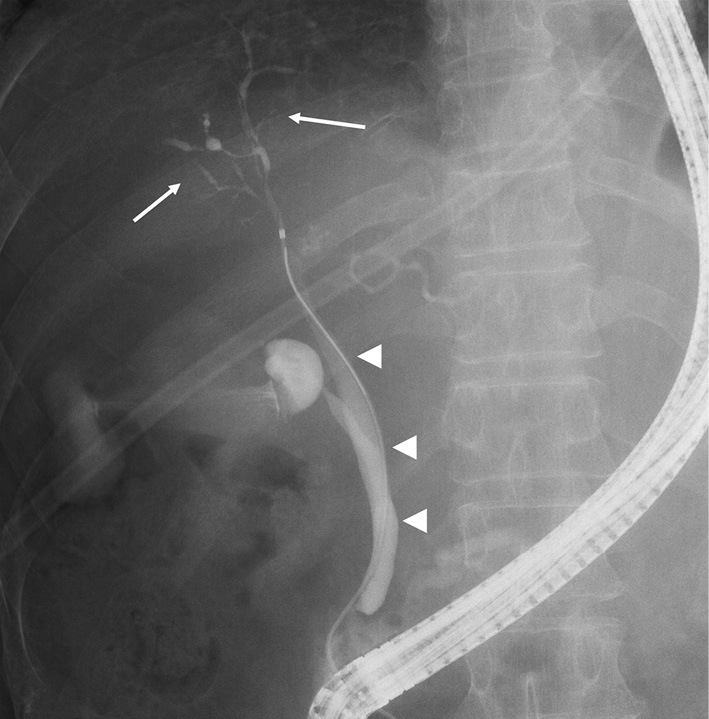
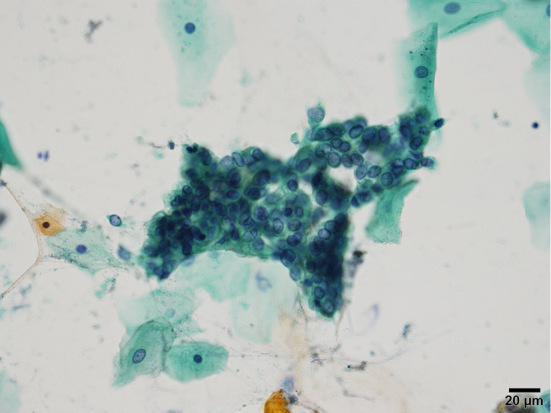
A 66-year-old man diagnosed with immunoglobulin G4-related sclerosing cholangitis (IgG4-SC) with diffuse intrahepatic bile duct stenosis and elevated serum IgG4 levels was referred for a further examination because of elevated serum carbohydrate antigen 19-9 levels despite treatment with corticosteroids. An umbilical nodule was found on a physical examination and a biopsy showed adenocarcinoma. Although several imaging studies revealed no changes from prior studies, bile cytology collected by endoscopic retrograde cholangiopancreatography showed adenocarcinoma. Consequently, the patient was diagnosed with cholangiocarcinoma resembling IgG4-SC after detecting an umbilical metastasis, also known as Sister Mary Joseph's nodule.
Keywords: Sister Mary Joseph's nodule; cholangiocarcinoma; immunoglobulin G4-related disease; immunoglobulin G4-related sclerosing cholangitis.
Conflict of interest statement
Figures
References
-
- Masamune A, Kikuta K, Hamada S, et al. . Nationwide epidemiological survey of autoimmune pancreatitis in Japan in 2016. J Gastroenterol 55: 462-470, 2020. - PubMed
-
- Nakazawa T, Kamisawa T, Okazaki K, et al. . Clinical diagnostic criteria for IgG4-related sclerosing cholangitis 2020: (Revision of the clinical diagnostic criteria for IgG4-related sclerosing cholangitis 2012). J Hepatobiliary Pancreat Sci 28: 235-242, 2021. - PubMed
-
- Nakazawa T, Naitoh I, Hayashi K, et al. . Diagnostic criteria for IgG4-related sclerosing cholangitis based on cholangiographic classification. J Gastroenterol 47: 79-87, 2012. - PubMed
-
- Mayo WJ. Metastasis in cancer. Proc Staff Meet Mayo Clin 3: 327, 1928.