

Current management of gastro-oesophageal reflux disease-treatment costs, safety profile, and effectiveness: a narrative review
- PMID: 37082451
- PMCID: PMC10112961
- DOI: 10.1093/gastro/goad008
Current management of gastro-oesophageal reflux disease-treatment costs, safety profile, and effectiveness: a narrative review
Abstract
Background: The purpose of this study was to review the current management of gastro-oesophageal reflux disease (GORD), including treatment costs, safety profile and effectiveness.
Methods: A literature review was performed of randomized-controlled trials, systematic reviews, Cochrane reports and National/Societal guidelines of the medical, endoscopic and surgical management of GORD. Proton pump inhibitor (PPI) prescribing patterns and expenditure were reviewed in different countries, including Australia, Canada, New Zealand, UK and USA.
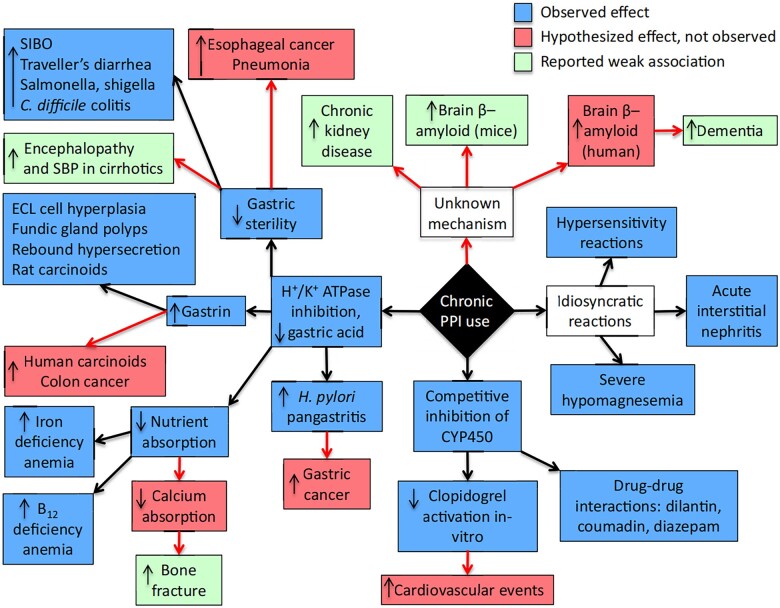
Results: Proton pump inhibitors (PPIs) are primarily indicated for control of GORD, Helicobacter pylori eradication (combined with antibiotics), preventing NSAID-induced gastrointestinal bleeding and treating peptic ulcer disease. There is widespread overprescribing of PPIs in Western and Eastern nations in terms of indication and duration, with substantial expense for national health providers. Despite a favourable short-term safety profile, there are observational associations of adverse effects with long-term PPIs. These include nutrient malabsorption, enteric infections and cardiovascular events. The prevalence of PPI use makes their long-term safety profile clinically relevant. Cost-benefit, symptom control and quality-of-life outcomes favour laparoscopic fundoplication rather than chronic PPI treatment. Laparoscopic fundoplication in long-term management of PPI-responsive GORD is supported by SAGES, NICE and ACG, and PPI-refractory GORD by AGA and SAGES guidelines. The importance of establishing a definitive diagnosis prior to invasive management is emphasized, especially in PPI-refractory heartburn.
Conclusions: We examined evidence-based guidelines for PPI prescribing and deprescribing in primary care and hospital settings and the need for PPI stewardship and education of health professionals. This narrative review presents the advantages and disadvantages of surgical, endoscopic and medical management of GORD, which may assist in shared decision making and treatment choice in individual patients.This paper was presented (GS020) at the 88th RACS Annual Scientific Conference, 6-10 May, 2019.
© The Author(s) 2023. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Conflict of interest statement
R.B.W. discloses relationships with Merck, Fisher and Paykel, Medtronic, and Ethicon involving funding for education, research, and attendance at scientific meetings.
Figures





Similar articles
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.Health Technol Assess. 2007 Dec;11(51):iii-iv, 1-164. doi: 10.3310/hta11510. Health Technol Assess. 2007. PMID: 18021578 Review.
-
Budget Impact of RefluxStop™ as a Treatment for Patients with Refractory Gastro-oesophageal Reflux Disease in the United Kingdom.J Health Econ Outcomes Res. 2024 Jan 11;11(1):1-7. doi: 10.36469/001c.90924. eCollection 2024. J Health Econ Outcomes Res. 2024. PMID: 38222857 Free PMC article.
-
A comparison of the cost effectiveness of pharmacotherapy or surgery (laparoscopic fundoplication) in the treatment of GORD.Pharmacoeconomics. 2007;25(10):829-41. doi: 10.2165/00019053-200725100-00003. Pharmacoeconomics. 2007. PMID: 17887805
-
Short-term cost effectiveness and long-term cost analysis comparing laparoscopic Nissen fundoplication with proton-pump inhibitor maintenance for gastro-oesophageal reflux disease.Br J Surg. 2005 Jun;92(6):700-6. doi: 10.1002/bjs.4933. Br J Surg. 2005. PMID: 15852426 Clinical Trial.
-
AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review.Gastroenterology. 2022 Apr;162(4):1334-1342. doi: 10.1053/j.gastro.2021.12.247. Epub 2022 Feb 17. Gastroenterology. 2022. PMID: 35183361 Review.
Cited by
-
Development and validation of a training course on proton pump inhibitor deprescription for general practitioners in a rural continuing medical education program: a pilot study.BMC Med Educ. 2024 Oct 27;24(1):1221. doi: 10.1186/s12909-024-06215-2. BMC Med Educ. 2024. PMID: 39465370 Free PMC article.
-
Current complementary and alternative therapy forgastroesophageal reflux disease.Gastroenterol Rep (Oxf). 2023 Oct 4;11:goad057. doi: 10.1093/gastro/goad057. eCollection 2023. Gastroenterol Rep (Oxf). 2023. PMID: 37810946 Free PMC article. Review.
-
Are PPI Unsafe for Pediatric Use?Glob Pediatr Health. 2024 Dec 11;11:2333794X241307187. doi: 10.1177/2333794X241307187. eCollection 2024. Glob Pediatr Health. 2024. PMID: 39670072 Free PMC article. No abstract available.
-
Clinical relevance of salivary pepsin detection in diagnosing gastroesophageal reflux disease subtypes.Gastroenterol Rep (Oxf). 2023 Sep 13;11:goad053. doi: 10.1093/gastro/goad053. eCollection 2023. Gastroenterol Rep (Oxf). 2023. PMID: 37720194 Free PMC article.
-
Diagnosis and treatment of patients with gastroesophageal reflux disease - a systematic review of cost-effectiveness and economic burden.BMC Health Serv Res. 2024 Nov 6;24(1):1351. doi: 10.1186/s12913-024-11781-8. BMC Health Serv Res. 2024. PMID: 39501242 Free PMC article.
References
-
- PBS Expenditure and Prescriptions. Australian Government Department of Health, Pharmaceutical Benefits Scheme (PBS). PBS Expenditure and Prescriptions, 2021. https://www.pbs.gov.au/info/statistics/expenditure-prescriptions/pbs-exp... (9 January 2022, date last accessed).
-
- Britt H, Miller GC, Henderson J, et al. General practice activity in Australia 2015–16. General Practice Series no. 40, 2016. https://ses.library.usyd.edu.au/bitstream/2123/15514/5/9781743325148_ONL... (9 January 2022, date last accessed).
-
- Hollingworth S, Duncan EL, Martin JH.. Marked increase in proton pump inhibitors use in Australia. Pharmacoepidem Drug Safe 2010;19:1019–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
