

Respiratory Syncytial Virus: A Comprehensive Review of Transmission, Pathophysiology, and Manifestation
- PMID: 37082497
- PMCID: PMC10111061
- DOI: 10.7759/cureus.36342
Respiratory Syncytial Virus: A Comprehensive Review of Transmission, Pathophysiology, and Manifestation
Abstract
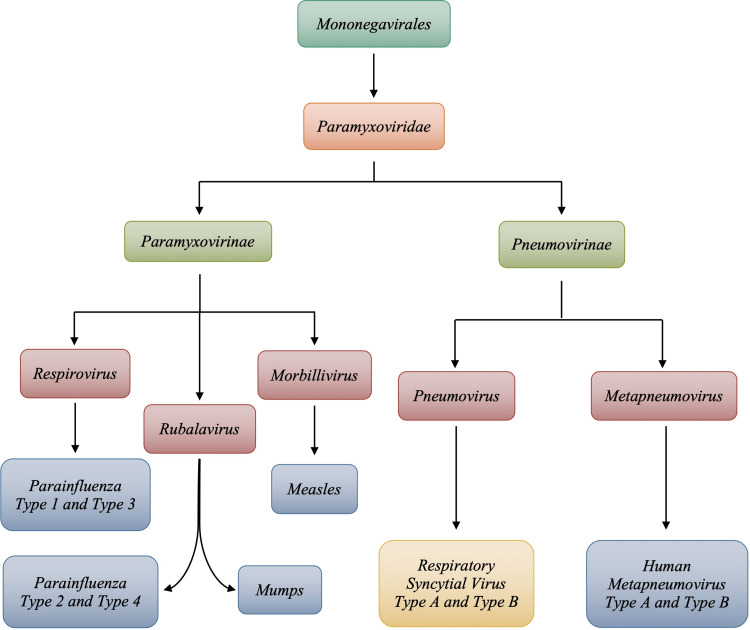
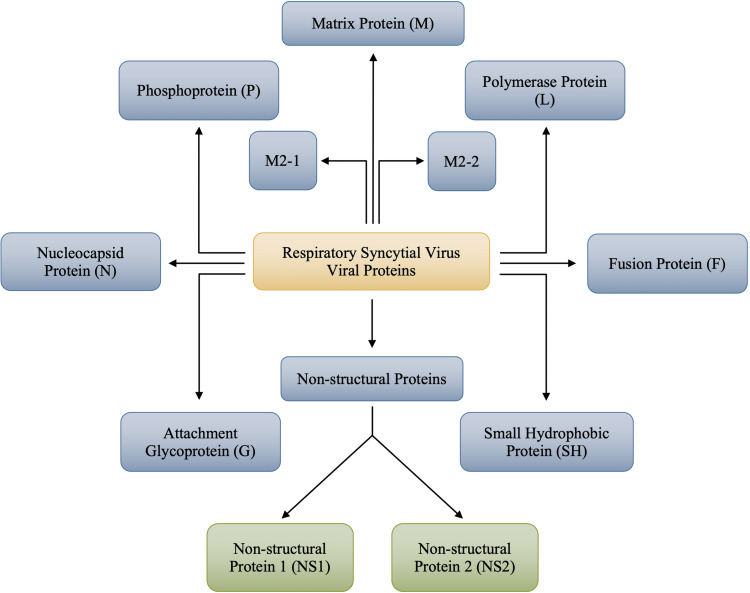
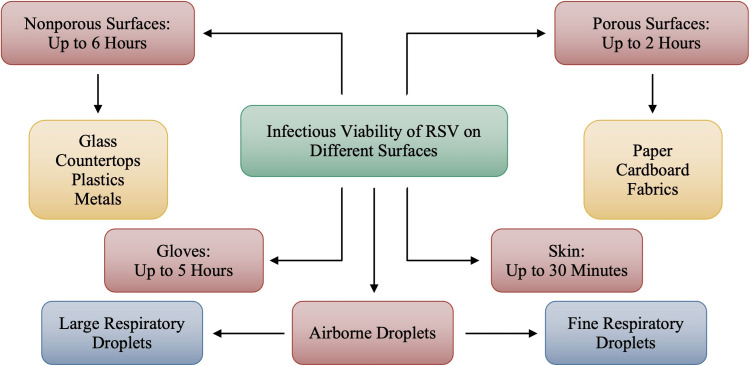
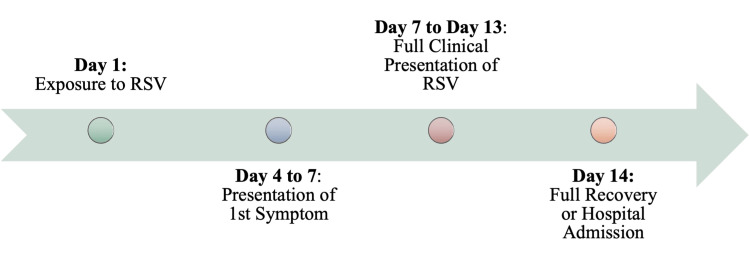
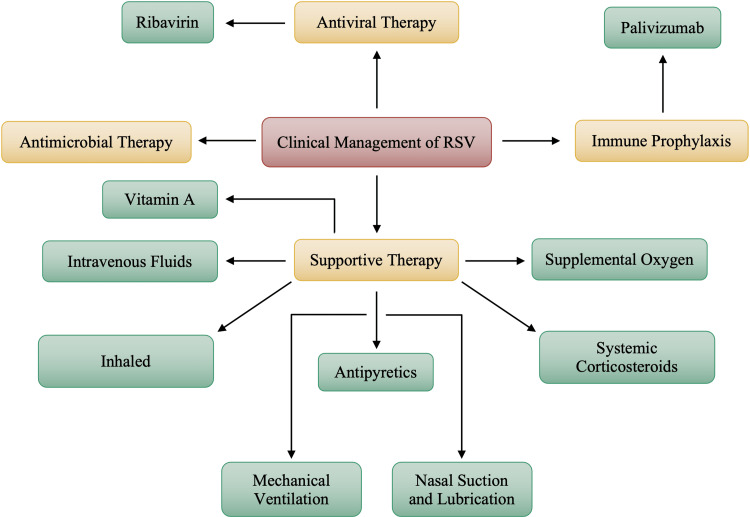
With an increasing global incidence in children younger than the age of five, respiratory syncytial virus (RSV) is one of the most common viral respiratory infections worldwide. Despite the increasing number of cases among infants and young children, RSV can infect any age group; however, some individuals are more high risk than others. Premature infants, young children, elderly, and immunocompromised individuals are the most likely to suffer a more severe presentation of RSV in comparison to healthy adults. RSV is transmitted through respiratory droplets via direct contact with an infected individual or with contaminated surfaces. The viral genome of RSV consists of 11 proteins. Out of these 11, two proteins allow for the attachment of the virus to the respiratory epithelial cells and fusion with host cells. Upon fusion, the viral material transfers to the host cell, where viral replication occurs. It is important to acknowledge that an individual is considered infectious and can transmit the virus even before the symptomatic presentation of RSV begins. As long as the individual is shedding the virus, he or she is considered infectious. The length of viral shedding also differs depending on the severity of the infection, who is infected, and the underlying immune status of an individual. Currently, there is no definitive treatment for RSV; however, supportive therapy is considered the mainstay treatment. Some pharmaceutical treatments such as ribavirin have been FDA-approved; however, the administration is typically limited to children and infants. Palivizumab is also administered as an immune prophylaxis; however, both therapies are constantly at the end of a cost-effective debate due to their extensively expensive nature and questionable adverse effect profiles. Supportive therapy includes hydration, supplemental oxygen, and mechanical ventilation in hospitalized cases; however, most RSV cases can be treated as outpatient cases. Prevention techniques such as hand washing and maintaining social distancing are imperative to minimize the transmission of the virus as much as remotely possible.
Keywords: paramyxoviridae; paramyxovirus; pathophysiology of rsv; pneumonia; respiratory syncytial virus.
Copyright © 2023, Kaler et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Jha A, Jarvis H, Fraser C, Openshaw P. SARS, MERS and other Viral Lung Infections. London, UK: European Respiratory Society; 2016. Respiratory syncytial virus; p. 38. - PubMed
-
- RSV transmission. [ Feb; 2023 ]. 2022. https://www.cdc.gov/rsv/about/transmission.html https://www.cdc.gov/rsv/about/transmission.html
-
- Respiratory syncytial virus infection in adults. Nam HH, Ison MG. BMJ. 2019;366:0. - PubMed
-
- RSV infections: state of the art. Piedimonte G. Cleve Clin J Med. 2015;82:0–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials