

Gradual and Remarkable Tumor Shrinkage Following Seven-Fraction Stereotactic Radiosurgery Alone With a Marginal Dose of 48.3 Gy for Large Lobar Possibly Intra-sulcal Brain Metastasis From Renal Cell Carcinoma
- PMID: 37082500
- PMCID: PMC10111507
- DOI: 10.7759/cureus.36346
Gradual and Remarkable Tumor Shrinkage Following Seven-Fraction Stereotactic Radiosurgery Alone With a Marginal Dose of 48.3 Gy for Large Lobar Possibly Intra-sulcal Brain Metastasis From Renal Cell Carcinoma
Abstract
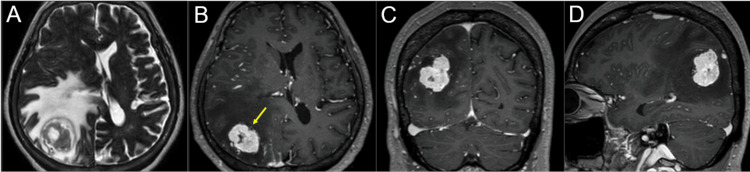
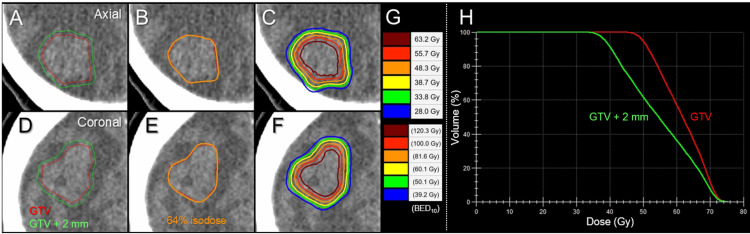
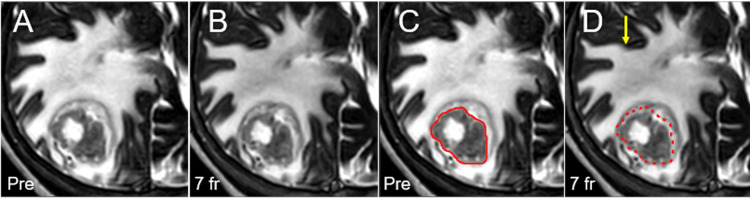
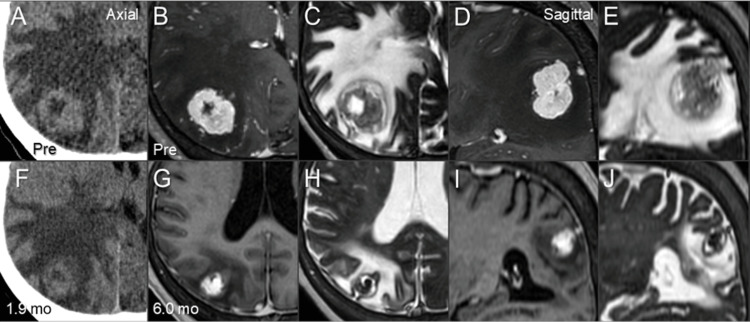
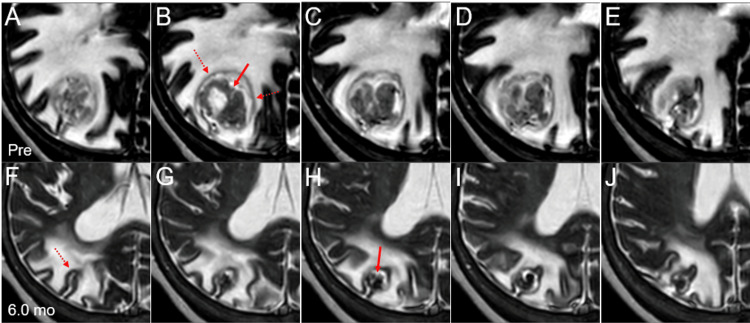
Brain metastases (BMs) from renal cell carcinoma (RCC) have the tendency of slow and insufficient tumor shrinkage along with prolongation of massive peritumoral edema following stereotactic radiosurgery (SRS). Herein, we describe a case of large lobar RCC-BM, with possible intra-sulcal location, treated with 7-fraction (fr) SRS without subsequent anti-cancer medication, which resulted in gradual and remarkable tumor shrinkage with extrication from the mass effect. A 59-year-old woman was incidentally diagnosed with bilateral RCC associated with multiple lung metastases and subsequently presented with symptomatic single BM of 32 mm in the maximum diameter (9.54 cm3) two months later while vacillating. A biopsy of the kidney showed clear cell carcinoma. The patient was deemed medically inoperable for BM due to unfit conditions, including severe deep venous thromboses and thrombocytopenia. Considering the tumor volume, irregular tumor configuration, non-superficial location, and mass effect, 98% of the gross tumor volume (GTV D98%) was covered by 48.3 Gy in 7 fr with 64% isodose. Dose distribution was optimized with volumetric modulated arcs with the affirmative allowance of very inhomogeneous GTV dose. Anti-cancer medication was limited to nivolumab plus ipilimumab followed by everolismus 12 days before and during SRS, respectively. Subsequently, the patient transitioned to palliative care due to a declining general condition. Although long-term administration of steroids was required, gradual and marked tumor shrinkage (1.25 cm3, 13.1% of the initial volume) and mitigation of the peritumoral edema was observed during six months after SRS. The main location of the initial BM was deemed as intra-sulcal in the intraparietal sulcus and originated in the cerebral cortex. The patient died nine months after SRS. The gradual but remarkable tumor response obtained with 7-fr SRS alone, in this case, provides a basis to further optimize fractionated SRS dosage to enhance efficacy and safety for large and/or symptomatic RCC-BMs not amenable to immediate surgical removal, in combination with anti-cancer pharmacotherapy, if feasible, including tyrosine kinase inhibitors, which may enhance efficacy against BM and mitigate adverse effects relevant to high dose SRS.
Keywords: brain metastasis; coagulopathy; fractionation; immune ckeckpoint inhibitor; large tumor; renal cell carcinoma; stereotactic radiosurgery; tyrosine kinase inhibitor; volumetric modulated arc-based radiosurgery.
Copyright © 2023, Ohtakara et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Pathologic complete response in renal cell carcinoma brain metastases treated with stereotactic radiosurgery. Teh BS, Bloch C, Paulino AC, et al. Clin Genitourin Cancer. 2007;5:334–337. - PubMed
-
- Gamma knife surgery for metastatic brain tumors from renal cell carcinoma. Shuto T, Inomori S, Fujino H, Nagano H. J Neurosurg. 2006;105:555–560. - PubMed
-
- Treatment strategy for metastatic brain tumors from renal cell carcinoma: selection of gamma knife surgery or craniotomy for control of growth and peritumoral edema. Shuto T, Matsunaga S, Suenaga J, Inomori S, Fujino H. J Neurooncol. 2010;98:169–175. - PubMed
-
- Stereotactic radiation therapy for renal cell carcinoma brain metastases in the tyrosine kinase inhibitors era: Outcomes of 120 patients. Klausner G, Troussier I, Biau J, et al. Clin Genitourin Cancer. 2019;17:191–200. - PubMed
Publication types
LinkOut - more resources
Full Text Sources