

Diagnostic accuracy of Xpert MTB/RIF Ultra and culture assays to detect Mycobacterium Tuberculosis using OMNIgene-sputum processed stool among adult TB presumptive patients in Uganda
- PMID: 37083706
- PMCID: PMC10121033
- DOI: 10.1371/journal.pone.0284041
Diagnostic accuracy of Xpert MTB/RIF Ultra and culture assays to detect Mycobacterium Tuberculosis using OMNIgene-sputum processed stool among adult TB presumptive patients in Uganda
Abstract
Background: Stool is a potential sample for diagnosing Mycobacterium tuberculosis (Mtb) in patients with difficulty in expectorating. However, high mycobacterial culture contamination rates and Xpert MTB/RIF Ultra test error rates on stool samples have limited its use. OMNIgene SPUTUM (OM-S) is a sample transport reagent with characteristics of sputum decontamination while maintaining viable Mtb. We evaluated the impact of OM-S on Mtb diagnostic yield from stool using smear microscopy, Xpert MTB/RIF Ultra, and culture among presumptive TB patients.
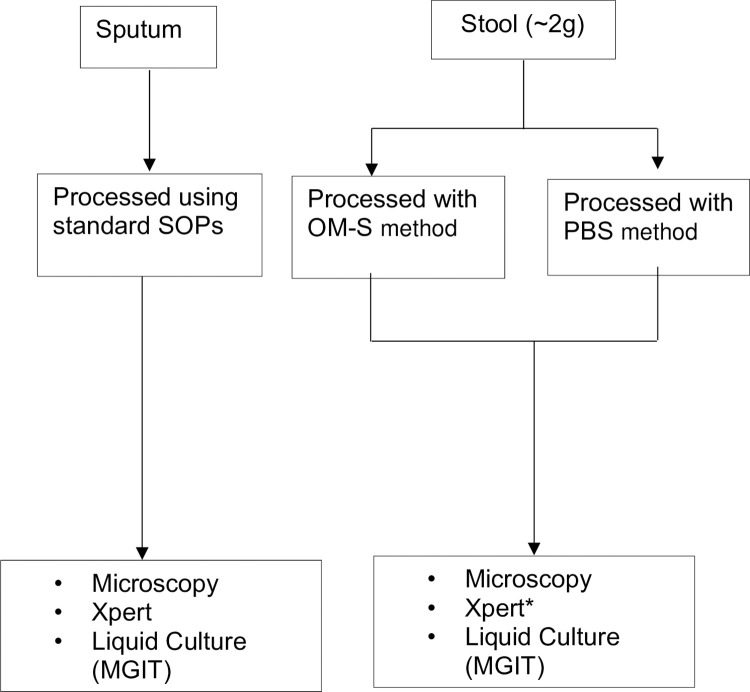
Methods: Paired stool and expectorated sputum samples were collected from consecutive Ugandan adults undergoing diagnostic evaluation for pulmonary TB between June 2018 and June 2019. Stool was divided into 2 portions: one was homogenized in OM-S (OM-S stool) and the other in PBS (PBS stool) as control. Both sputum and processed stool were tested for Mtb using concentrated smear fluorescence microscopy (CFM), Xpert MTB/RIF Ultra (Xpert) and Mycobacteria Growth Indicator Tube (MGIT) culture. Sensitivity, specificity, and predictive values for each test were calculated against sputum MGIT culture as the reference standard.
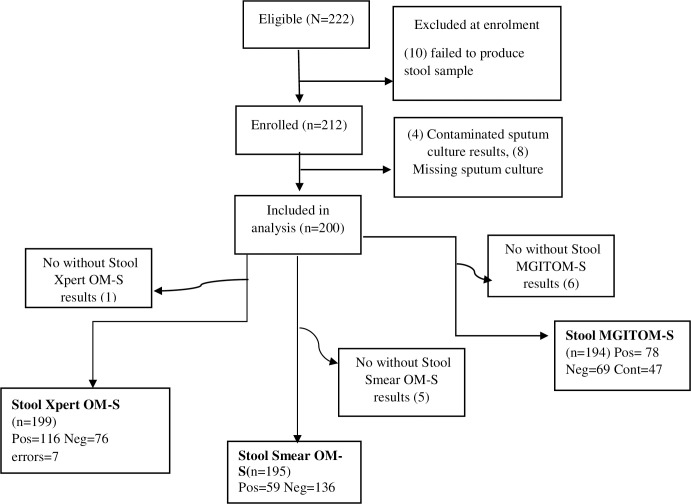
Results: Of the 200 participants, 120 (60%) were male, 73 (37%) were HIV positive (median CD4 120 cells/uL (IQR 43-297)) and 128 (64%) had confirmed pulmonary TB by sputum MGIT culture. Seven (4%) OM-S stool Xpert samples reported errors while 47 (25%) and 103 (61%) were contaminated on OM-S stool MGIT and PBS stool MGIT, respectively. OM-S stool MGIT was able to accurately diagnose 56 of the contaminated PBS stool MGIT samples compared to only 5 of the contaminated OM-S stool MGIT samples diagnosed by PBS stool MGIT. Sensitivity (95% Confidence Interval, CI) 89% (83-94) for OM-S stool Xpert was higher compared to that of OM-S stool MGIT 60% (51-69) and PBS stool MGIT 42% (32-52). Specificity (95%CI) 91% (82-97) was also higher for OM-S stool Xpert compared to OM-S stool MGIT 64% (51-75) and PBS stool MGIT 26% (16-38).
Conclusion: Stool processed with OM-S showed potential to improve Mtb diagnostic yield and reduce rates of indeterminate results when tested on Xpert and MGIT culture. The method may thus be of value in Mtb detection among patients with difficulty to expectorate.
Copyright: © 2023 Sessolo et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Investigation of OMNIgene·SPUTUM performance in delayed tuberculosis testing by smear, culture, and Xpert MTB/RIF assays in Uganda.J Epidemiol Glob Health. 2017 Jun;7(2):103-109. doi: 10.1016/j.jegh.2017.04.001. Epub 2017 Apr 13. J Epidemiol Glob Health. 2017. PMID: 28413105 Free PMC article.
-
High Mycobacterium tuberculosis Bacillary Loads Detected by Tuberculosis Molecular Bacterial Load Assay in Patient Stool: a Potential Alternative for Nonsputum Diagnosis and Treatment Response Monitoring of Tuberculosis.Microbiol Spectr. 2022 Feb 23;10(1):e0210021. doi: 10.1128/spectrum.02100-21. Epub 2022 Jan 12. Microbiol Spectr. 2022. PMID: 35019686 Free PMC article.
-
Xpert MTB/RIF assay in the diagnosis of pulmonary tuberculosis in children in tertiary care setting in South India.J Trop Pediatr. 2024 Aug 10;70(5):fmae024. doi: 10.1093/tropej/fmae024. J Trop Pediatr. 2024. PMID: 39152039
-
Xpert MTB/RIF and Xpert Ultra assays for screening for pulmonary tuberculosis and rifampicin resistance in adults, irrespective of signs or symptoms.Cochrane Database Syst Rev. 2021 Mar 23;3(3):CD013694. doi: 10.1002/14651858.CD013694.pub2. Cochrane Database Syst Rev. 2021. PMID: 33755189 Free PMC article.
-
Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults.Cochrane Database Syst Rev. 2019 Jun 7;6(6):CD009593. doi: 10.1002/14651858.CD009593.pub4. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2021 Feb 22;2:CD009593. doi: 10.1002/14651858.CD009593.pub5. PMID: 31173647 Free PMC article. Updated.
Cited by
-
Xpert MTB/RIF Ultra assay for pulmonary tuberculosis and rifampicin resistance in adults and adolescents.Cochrane Database Syst Rev. 2025 Jul 29;7(7):CD009593. doi: 10.1002/14651858.CD009593.pub6. Cochrane Database Syst Rev. 2025. PMID: 40728034 Free PMC article.
-
Performance of stool Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis among adults living with HIV: a multicentre, prospective diagnostic study.Lancet Microbe. 2025 Jul;6(7):101085. doi: 10.1016/j.lanmic.2025.101085. Epub 2025 Apr 4. Lancet Microbe. 2025. PMID: 40194533 Free PMC article.
-
Performance of a stool-based quantitative PCR assay for the diagnosis of tuberculosis in adolescents and adults: a multinational, prospective diagnostic accuracy study.Lancet Microbe. 2024 May;5(5):e433-e441. doi: 10.1016/S2666-5247(23)00391-9. Epub 2024 Mar 7. Lancet Microbe. 2024. PMID: 38461830 Free PMC article.
-
Non-sputum-based samples and biomarkers for detection of Mycobacterium tuberculosis: the hope to improve childhood and HIV-associated tuberculosis diagnosis.Eur J Med Res. 2024 Oct 18;29(1):502. doi: 10.1186/s40001-024-02092-z. Eur J Med Res. 2024. PMID: 39420420 Free PMC article. Review.
-
Diagnostic accuracy of Xpert MTB/RIF Ultra for detecting pulmonary tuberculosis and rifampicin resistance: a systematic review and meta-analysis.Eur J Clin Microbiol Infect Dis. 2025 Mar;44(3):681-702. doi: 10.1007/s10096-024-05032-1. Epub 2025 Jan 4. Eur J Clin Microbiol Infect Dis. 2025. PMID: 39754613
References
-
- World Health Organization, ‘Global tuberculosis report 2020. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO.’, vol. 2020, 2020.
-
- World Health Organization, ‘Global tuberculosis report 2019. Geneva: World Health Organization; 2019. Licence: CC BY-NCSA 3.0 IGO’, vol. 2019, 2019.
-
- Hartung T, Maulu A, Nash J, Fredlund V., ‘Suspected pulmonary tuberculosis in rural South Africa-Sputum induction as a simple diagnostic tool? South African Medical Journal. 2002;92(6):455–458’, vol. 2002;92(6):455–458, 2002. - PubMed
-
- Bates M O ’Grady J, Maeurer M, et al.., ‘Assessment of the Xpert MTB/RIF assay for diagnosis of tuberculosis with gastric lavage aspirates in children in sub-Saharan Africa: a prospective descriptive study. The Lancet infectious diseases. 2013;13(1):36–42.’, 2013. doi: 10.1016/S1473-3099(12)70245-1 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
