

Visceral Metastasis Predicts Response to New Hormonal Agents in Metastatic Castration-Sensitive Prostate Cancer
- PMID: 37084289
- PMCID: PMC10322122
- DOI: 10.1093/oncolo/oyad102
Visceral Metastasis Predicts Response to New Hormonal Agents in Metastatic Castration-Sensitive Prostate Cancer
Abstract
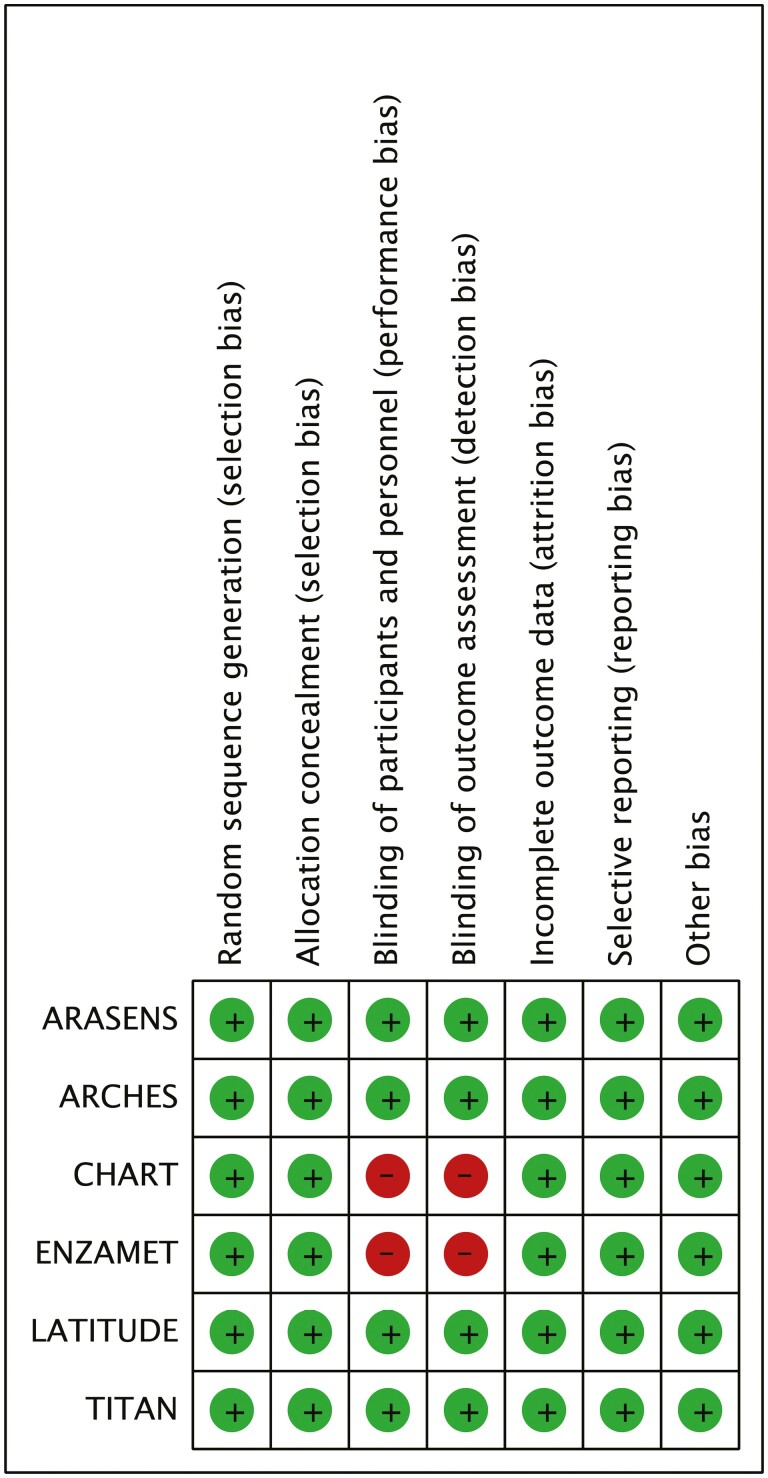
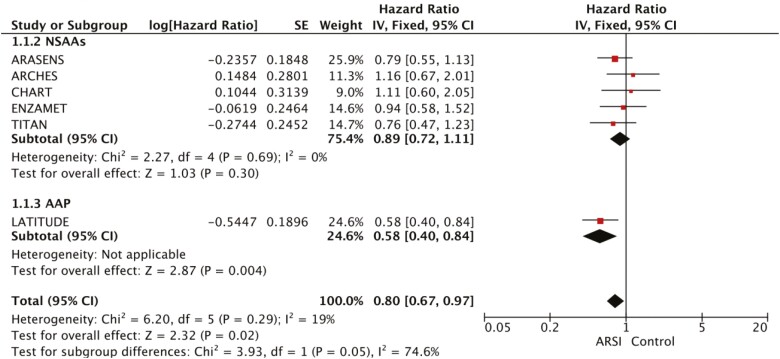
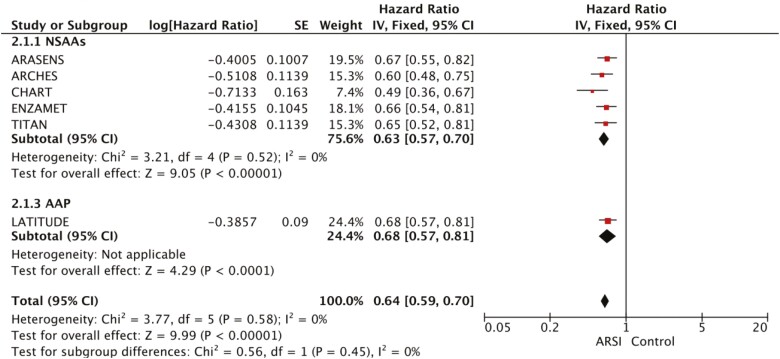
Visceral metastasis (VM) and a higher number of bone metastasis generally define high volume/risk in patients with metastatic castration-sensitive prostate cancer (mCSPC). Subgroup analysis of pivotal trials did not show a clear benefit of second-generation non-steroidal anti-androgens (NSAAs) in patients with VM. However, subgroup analysis of the trial assessing abiraterone acetate, a CYP 17 inhibitor, plus prednisone (AAP) showed an improved overall survival (OS) in patients with mCSPC with VM. We searched MEDLINE, Web of Science, and congress abstracts for the phase III randomized controlled trials of second-generation NSAAs and AAP in patients with mCSPC. In this pooled analysis, we included 6485 patients from the 6 phase III trials. The rate of patients with VM was 15.2%. Interestingly, in contrast to NSAAs, AAP seems to be effective in improving OS among patients with VM (hazard ratio, HR: 0.89, 95% CI, 0.72-1.11, P = .30 for second-generation NSAAs; HR: 0.58, 95% CI, 0.40-0.84, P = .004 for AAP). In contrast, both second-generation NSAAs (HR: 0.63, 95% CI, 0.57-0.70, P < .001) and AAP (HR: 0.68, 95% CI, 0.57-0.81, P < .001) improved OS in patients without VM. In this pooled analysis, we demonstrate that while AAP provided an OS improvement in patients with VM, second-generation NSAAs did not demonstrate a similar OS benefit in this population.
Keywords: abiraterone acetate; castration-sensitive; non-steroidal anti-androgens; prostate cancer.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
Rana R. McKay reported consulting or advisory role for AstraZeneca, Aveo, Bayer, BMS, Calithera, Caris, Dendreon, Exelixis, Janssen, Merck, Myovant, Novartis, Pfizer, Sanofi, Sorrento Therapeutics, Seagen, Tempus, and Telix and research funding from Bayer, AstraZeneca, Oncternal, Tempus. Silke Gillessen reported consulting or advisory role for Sanofi, Orion, Roche, Amgen, AstraZeneca, Novartis, Myriad Genetics, and MSD; honoraria from Televisione Svizzera Italiana; invited speaker for ESMO, SAKK, SAMO, Orikata Academy Research Group, China Anti-Cancer Association Genitourinary Oncology Committee, S. Grasso Consulting, and Deso; speaker’s bureau for Janssen Cilag; travel grant from ProteoMEdiX and AstraZeneca; institutional honoraria for advisory boards and Independent Data Monitoring or Steering Committees for Bayer, Janssen Cilag, Roche, AAA International, Amgen, Menarini Silicon Biosystems, Astellas Pharma, Tolero Pharmaceuticals, MSD, Pfizer, Telixpharma, BMS, and Orion; honoraria for the institution from WedMed-Medscape; patent royalties and other intellectual property for a research method for biomarker WO2009138392. Toni K. Choueiri reported institutional and personal support, paid and unpaid support for research, participating in advisory boards, consultancy, and honoraria from AstraZeneca, Aravive, Aveo, Bayer, Bristol Myers Squibb, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVA, Infinity, Ipsen, Jansen, Kanaph, Lilly, Merck, Nikang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, UpToDate, and CME events (Peerview, OncLive, and MJH), outside the submitted work; institutional patents filed on molecular mutations, immunotherapy response and toxicity, and ctDNA; equity in Tempest, Pionyr, Osel, Precede Bio; being part of committees in the National Comprehensive Cancer Network, GU Steering Committee, American Society of Clinical Oncology, European Society for Medical Oncology, Academic and Community Cancer Research United, and KidneyCAN; having mentored several non-US citizens on research projects partly funded by non-US sources; and additional independent funding from drug companies or royalties for research around the subject matter paid to institution. Yüksel Ürün reported receipt of honoraria or consultation fees from Astellas, AstraZeneca, Bristol-Myers Squibb, Janssen Oncology, MSD, Pfizer, and Roche; participation in a company-sponsored speaker’s bureau for Astellas, Amgen, AstraZeneca, Bristol-Myers Squibb, Janssen Oncology, Pfizer, and Roche. Emre Yekedüz indicated no financial relationships.
Figures
Similar articles
-
Impact of abiraterone acetate plus prednisone in patients with castration-sensitive prostate cancer and visceral metastases over four years of follow-up: A post-hoc exploratory analysis of the LATITUDE study.Eur J Cancer. 2022 Feb;162:56-64. doi: 10.1016/j.ejca.2021.11.026. Epub 2021 Dec 23. Eur J Cancer. 2022. PMID: 34953443 Clinical Trial.
-
Patient-reported outcomes following abiraterone acetate plus prednisone added to androgen deprivation therapy in patients with newly diagnosed metastatic castration-naive prostate cancer (LATITUDE): an international, randomised phase 3 trial.Lancet Oncol. 2018 Feb;19(2):194-206. doi: 10.1016/S1470-2045(17)30911-7. Epub 2018 Jan 8. Lancet Oncol. 2018. PMID: 29326030 Clinical Trial.
-
Association between concomitant proton pump inhibitor use and survival of patients with metastatic prostate cancer receiving abiraterone acetate: a post-hoc analysis of pooled data from three randomized controlled trials.Prostate Cancer Prostatic Dis. 2024 Sep;27(3):444-450. doi: 10.1038/s41391-023-00695-x. Epub 2023 Jul 18. Prostate Cancer Prostatic Dis. 2024. PMID: 37464102
-
Predictors of efficacy of androgen-receptor-axis-targeted therapies in patients with metastatic castration-sensitive prostate cancer: A systematic review and meta-analysis.Crit Rev Oncol Hematol. 2020 Jul;151:102992. doi: 10.1016/j.critrevonc.2020.102992. Epub 2020 May 23. Crit Rev Oncol Hematol. 2020. PMID: 32474391
-
Abiraterone acetate in combination with prednisone in the treatment of prostate cancer: safety and efficacy.Expert Rev Anticancer Ther. 2020 Aug;20(8):629-638. doi: 10.1080/14737140.2020.1785289. Epub 2020 Jun 25. Expert Rev Anticancer Ther. 2020. PMID: 32552120 Review.
Cited by
-
Prostate Cancer Liver Metastasis: An Ominous Metastatic Site in Need of Distinct Management Strategies.J Clin Med. 2024 Jan 27;13(3):734. doi: 10.3390/jcm13030734. J Clin Med. 2024. PMID: 38337427 Free PMC article. Review.
-
Real-world retrospective study of prostate-specific antigen and safety assessment with darolutamide plus androgen deprivation therapy for metastasis hormone-sensitive prostate cancer.Transl Androl Urol. 2024 Mar 31;13(3):433-441. doi: 10.21037/tau-24-96. Epub 2024 Mar 25. Transl Androl Urol. 2024. PMID: 38590967 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
