

American Indians travel great distances for obstetrical care: Examining rural and racial disparities
- PMID: 37084704
- PMCID: PMC10164064
- DOI: 10.1016/j.socscimed.2023.115897
American Indians travel great distances for obstetrical care: Examining rural and racial disparities
Abstract
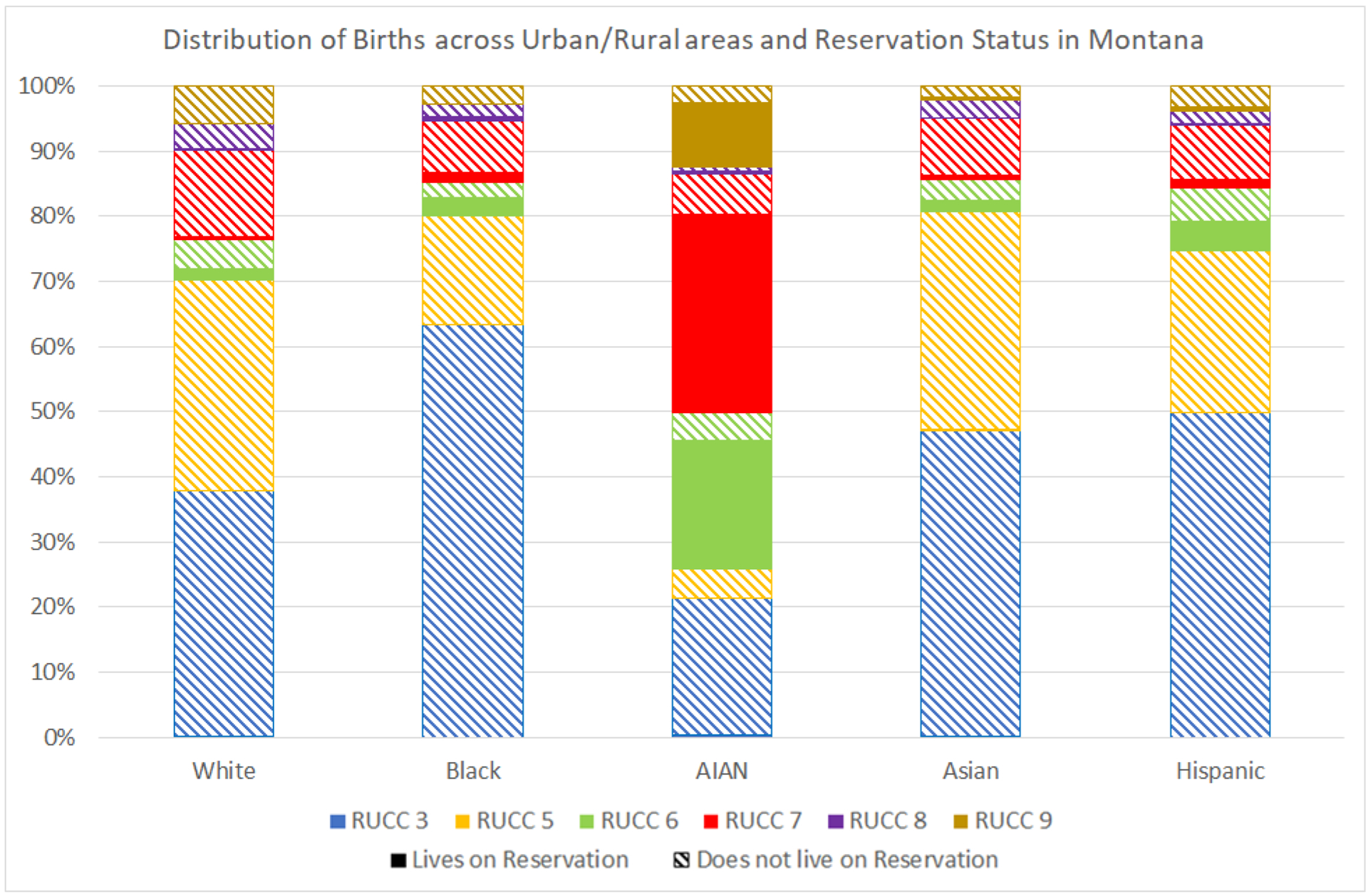
Rural, American Indian/Alaska Native (AI/AN) people, a population at elevated risk for complex pregnancies, have limited access to risk-appropriate obstetric care. Obstetrical bypassing, seeking care at a non-local obstetric unit, is an important feature of perinatal regionalization that can alleviate some challenges faced by this rural population, at the cost of increased travel to give birth. Data from five years (2014-2018) of birth certificates from Montana, along with the 2018 annual survey of the American Hospital Association (AHA) were used in logistic regression models to identify predictors of bypassing, with ordinary least squares regression models used to predict factors associated with the distance (in miles) birthing people drove beyond their local obstetric unit to give birth. Logit analyses focused on hospital-based births to Montana residents delivered during this time period (n = 54,146 births). Distance analyses focused on births to individuals who bypassed their local obstetric unit to deliver (n = 5,991 births). Individual-level predictors included maternal sociodemographic characteristics, location, perinatal health characteristics, and health care utilization. Facility-related measures included level of obstetric care of the closest and delivery hospitals, and distance to the closest hospital-based obstetric unit. Findings suggest that birthing people living in rural areas and on American Indian reservations were more likely to bypass to give birth, with bypassing likelihood depending on health risk, insurance, and rurality. AI/AN and reservation-dwelling birthing people traveled significantly farther when bypassing. Findings highlight that distance traveled was even farther for AI/AN people facing pregnancy health risks (23.8 miles farther than White people with pregnancy risks) or when delivering at facilities offering complex care (14-44 miles farther than White people). While bypassing may connect rural birthing people to more risk-appropriate care, rural and racial inequities in access persist, with rural, reservation-dwelling AI/AN birthing people experiencing greater likelihood of bypassing and traveling greater distances when bypassing.
Keywords: Access/demand/utilization of services; American Indians; Birthing people; Health care disparities; Montana; Obstetrics/gynecology; Racial/ethnic differences in health and health care; Rural health.
Published by Elsevier Ltd.
Conflict of interest statement
Declarations of competing interest None.
Figures
Similar articles
-
Navigating geographical disparities: access to obstetric hospitals in maternity care deserts and across the United States.BMC Pregnancy Childbirth. 2024 May 8;24(1):350. doi: 10.1186/s12884-024-06535-7. BMC Pregnancy Childbirth. 2024. PMID: 38720255 Free PMC article.
-
Evaluating disparities in access to obstetric services for American Indian women across Montana.J Rural Health. 2022 Jan;38(1):151-160. doi: 10.1111/jrh.12572. Epub 2021 Mar 23. J Rural Health. 2022. PMID: 33754411 Free PMC article.
-
Bypassing of nearest labor & delivery unit is contingent on rurality, wealth, and race.Birth. 2023 Mar;50(1):5-10. doi: 10.1111/birt.12712. Epub 2023 Feb 8. Birth. 2023. PMID: 36752116
-
Rural hospital and obstetric unit closures as social determinants of racial and ethnic maternal health disparities: A scoping review.J Adv Nurs. 2024 Aug;80(8):3059-3071. doi: 10.1111/jan.16005. Epub 2023 Dec 2. J Adv Nurs. 2024. PMID: 38041583
-
Racial and Ethnic Disparities in Preterm Birth Among American Indian and Alaska Native Women.Matern Child Health J. 2016 Jan;20(1):16-24. doi: 10.1007/s10995-015-1803-1. Matern Child Health J. 2016. PMID: 26187576 Review.
Cited by
-
The Availability of Midwifery Care in Rural United States Communities.J Midwifery Womens Health. 2024 Nov-Dec;69(6):929-936. doi: 10.1111/jmwh.13676. Epub 2024 Jul 23. J Midwifery Womens Health. 2024. PMID: 39044450 Free PMC article.
-
Obstetric care in rural critical access hospitals: A domestic application of the World Health Organization Emergency Obstetric Care framework in rural communities.J Rural Health. 2025 Mar;41(2):e70037. doi: 10.1111/jrh.70037. J Rural Health. 2025. PMID: 40411254 Free PMC article.
-
Navigating geographical disparities: access to obstetric hospitals in maternity care deserts and across the United States.BMC Pregnancy Childbirth. 2024 May 8;24(1):350. doi: 10.1186/s12884-024-06535-7. BMC Pregnancy Childbirth. 2024. PMID: 38720255 Free PMC article.
-
Inferred Attractiveness Gravity-Based Models for Estimating Realized Access at Rural Hospitals.J Oper Res Soc. 2025;76(5):984-999. doi: 10.1080/01605682.2024.2406236. Epub 2024 Sep 25. J Oper Res Soc. 2025. PMID: 40453422
-
The implications of using maternity care deserts to measure progress in access to obstetric care: a mixed-integer optimization analysis.BMC Health Serv Res. 2024 May 30;24(1):682. doi: 10.1186/s12913-024-11135-4. BMC Health Serv Res. 2024. PMID: 38811929 Free PMC article.
References
-
- Tomkins L Thrown a lifeline. How Medicaid is rebuilding healthcare on Fort Belknap. Native News. The University of Montana School of Journalism; 2017(26):4–9. https://nativenews.jour.umt.edu/2017/thrown-lifeline-fort-belknap/
-
- March of Dimes. Nowhere To Go: Maternity Care Deserts Across the U.S 2020. https://www.marchofdimes.org/materials/2020-Maternity-Care-Report.pdf
-
- Rayburn WF, Richards ME, Elwell EC. Drive times to hospitals with perinatal care in the United States. Obstetrics & Gynecology. 2012;119(3):611–616. - PubMed
-
- Von Reichert C, McBroom WH, Reed FW, Wilson PB. Access to health care and travel for birthing: Native American-White differentials in Montana. Geoforum. 1995;26(3):297–308.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
