

Genomic mapping of metastatic organotropism in lung adenocarcinoma
- PMID: 37084736
- PMCID: PMC10391526
- DOI: 10.1016/j.ccell.2023.03.018
Genomic mapping of metastatic organotropism in lung adenocarcinoma
Abstract
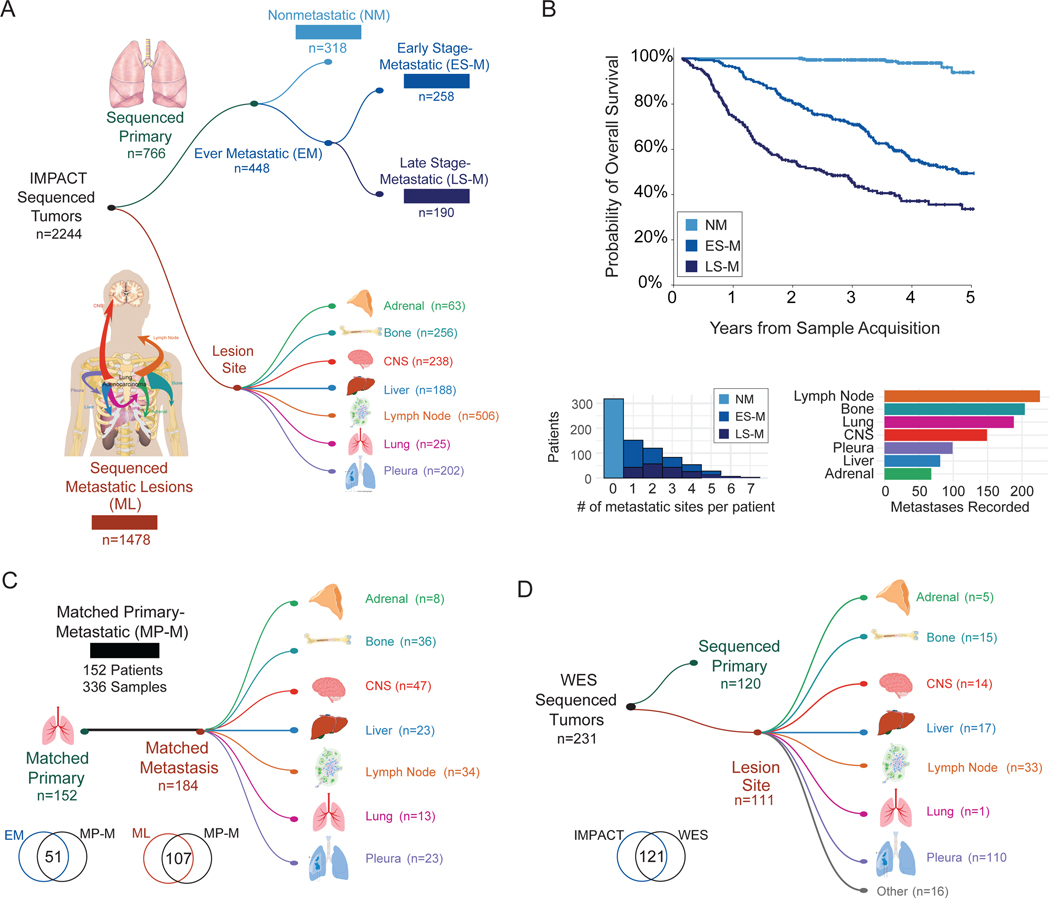
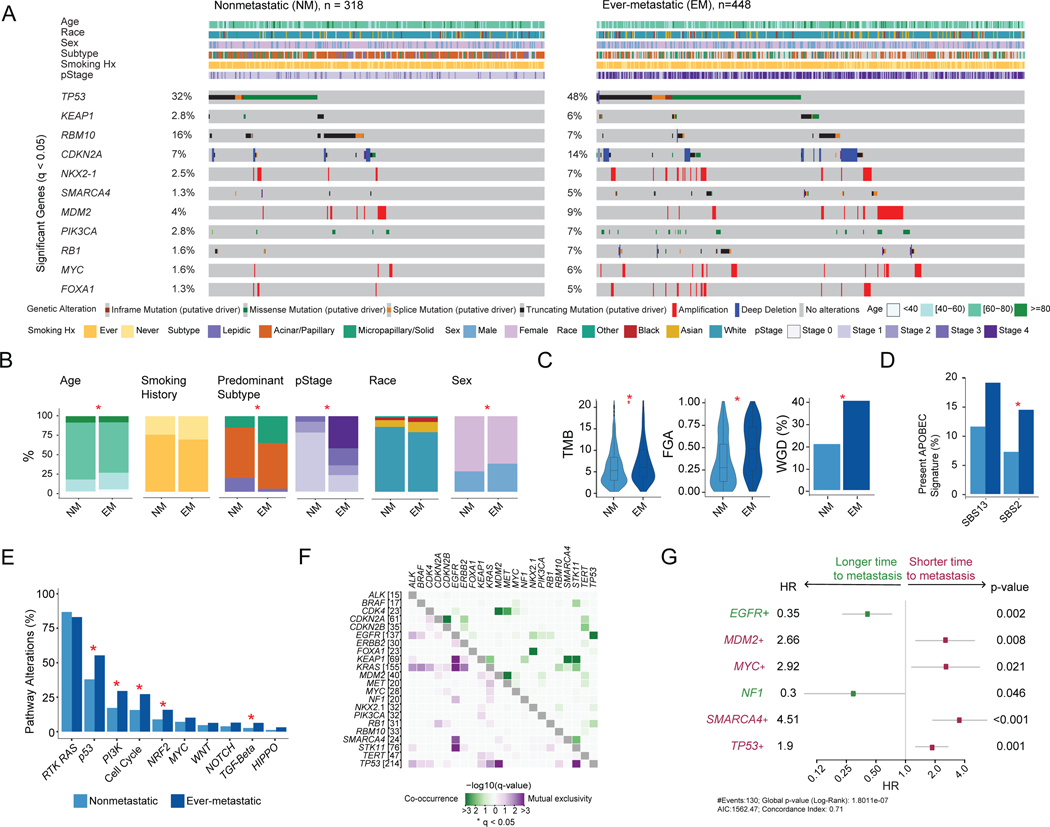
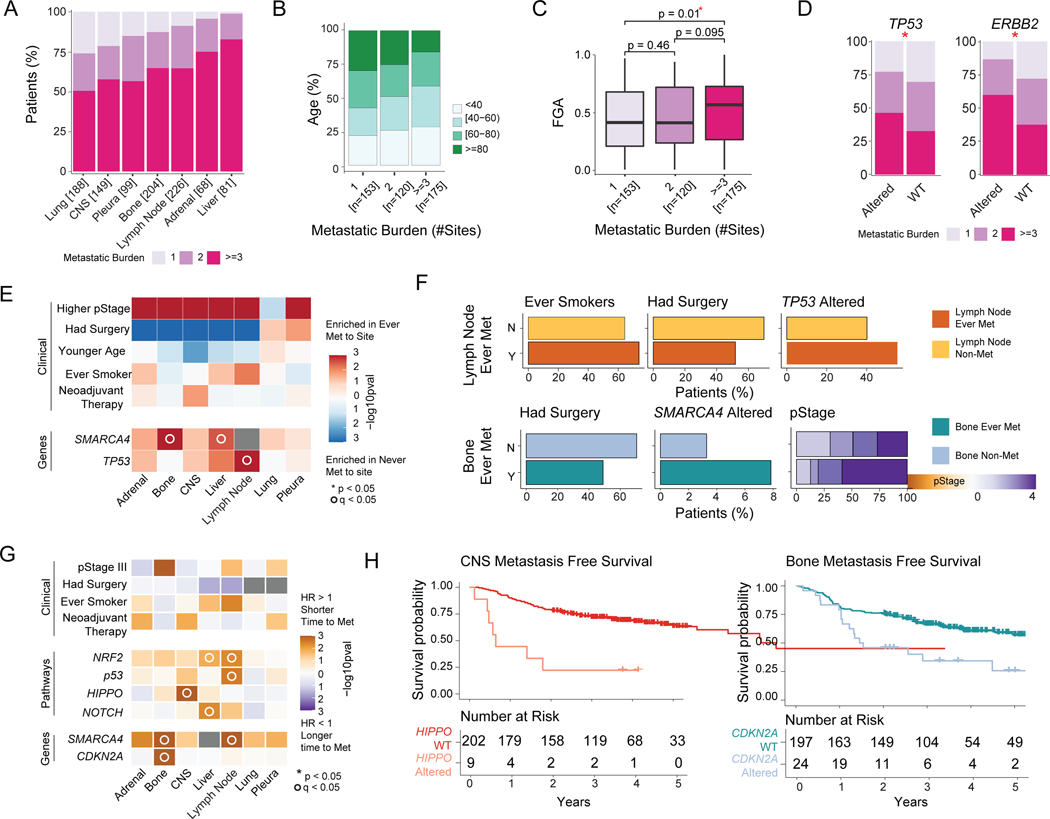
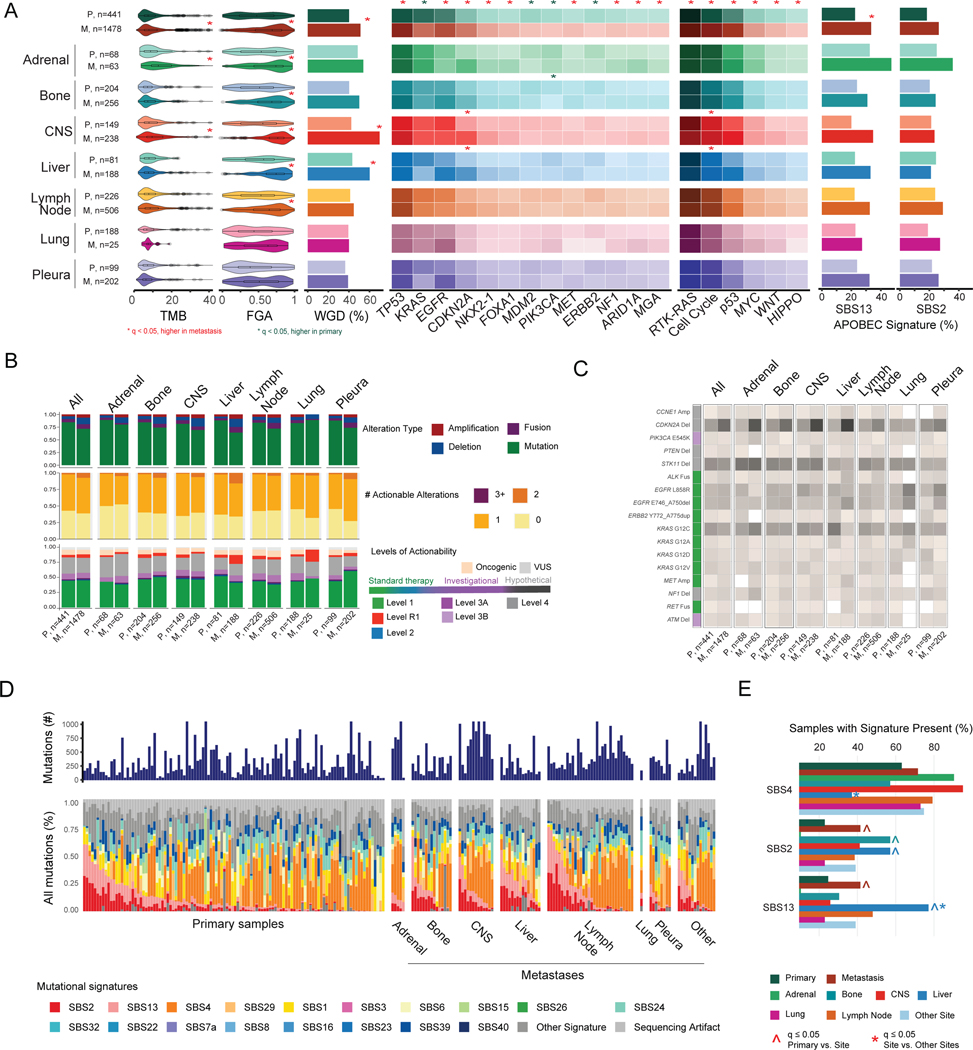
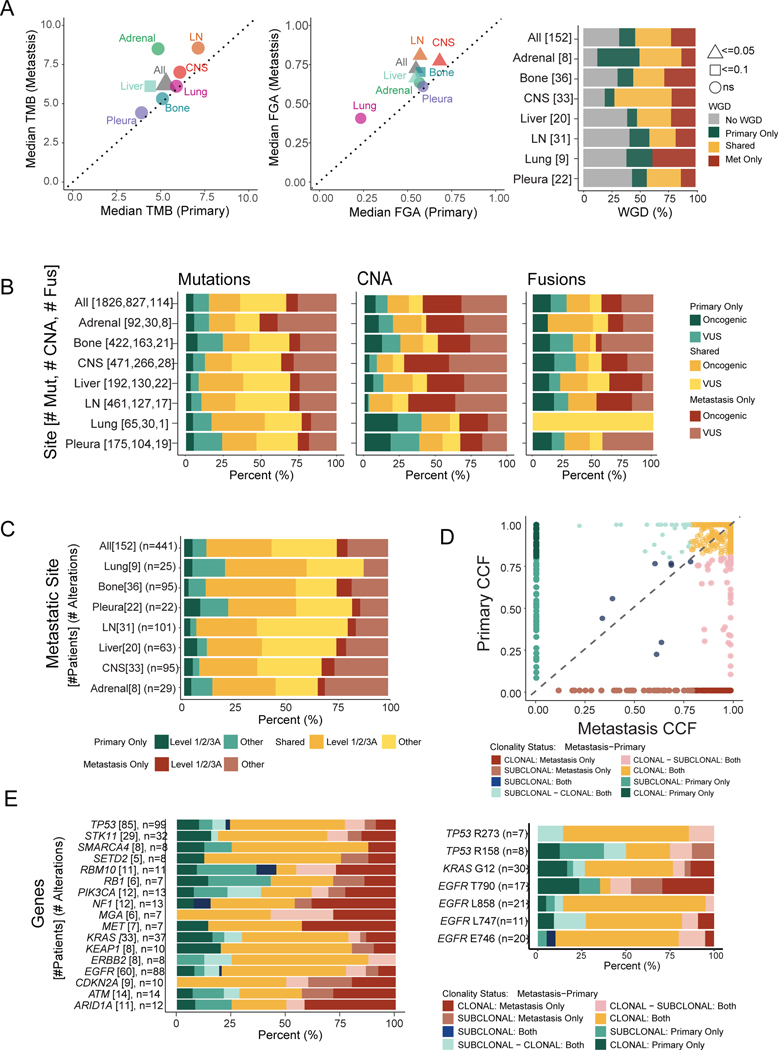
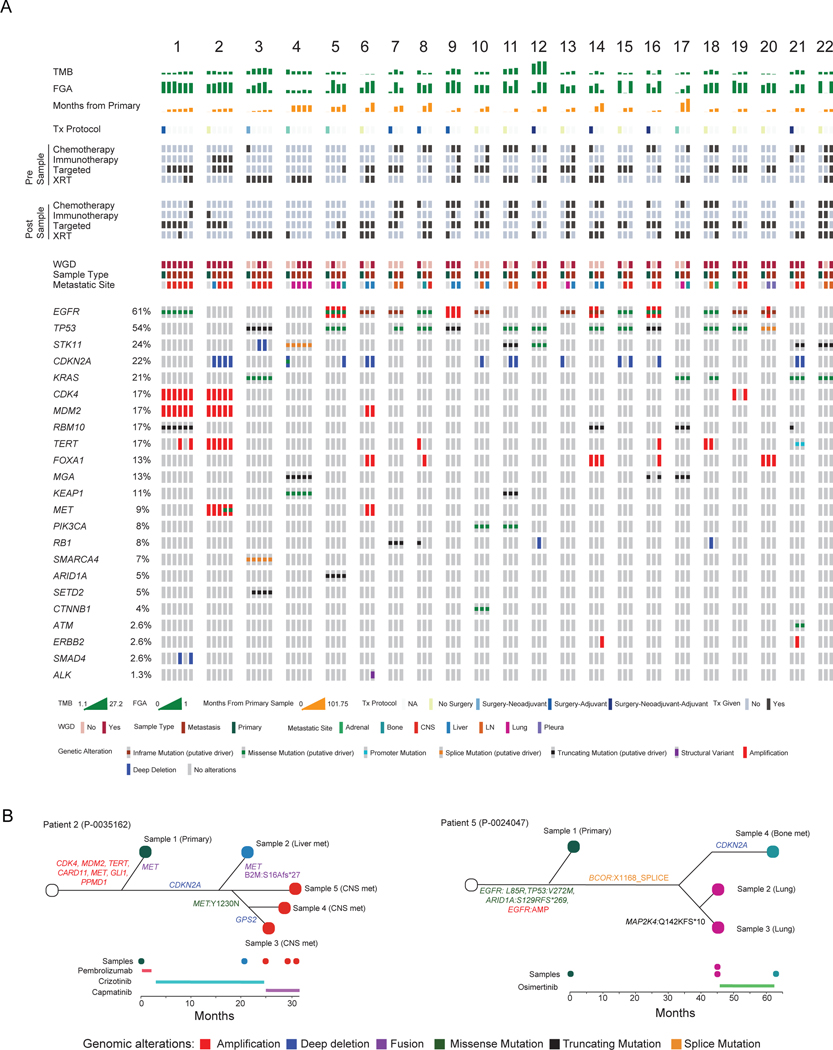
We analyzed 2,532 lung adenocarcinomas (LUAD) to identify the clinicopathological and genomic features associated with metastasis, metastatic burden, organotropism, and metastasis-free survival. Patients who develop metastasis are younger and male, with primary tumors enriched in micropapillary or solid histological subtypes and with a higher mutational burden, chromosomal instability, and fraction of genome doublings. Inactivation of TP53, SMARCA4, and CDKN2A are correlated with a site-specific shorter time to metastasis. The APOBEC mutational signature is more prevalent among metastases, particularly liver lesions. Analyses of matched specimens show that oncogenic and actionable alterations are frequently shared between primary tumors and metastases, whereas copy number alterations of unknown significance are more often private to metastases. Only 4% of metastases harbor therapeutically actionable alterations undetected in their matched primaries. Key clinicopathological and genomic alterations in our cohort were externally validated. In summary, our analysis highlights the complexity of clinicopathological features and tumor genomics in LUAD organotropism.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests C.M.R. has consulted regarding oncology drug development with AbbVie, Amgen, Astra Zeneca, Epizyme, Genentech/Roche, Ipsen, Jazz, Lilly, and Syros and serves on the scientific advisory boards of Bridge Medicines, Earli, and Harpoon Therapeutics. G.J.R. has institutional research funding from Mirait, Takeda, Merck, Roche, Novartis, and Pfizer. D.B.S. has consulted for and received honoraria from Pfizer, Lilly/Loxo Oncology, Vividion Therapeutics, Scorpion Therapeutics, and BridgeBio. M.F.B. has consulted for Eli Lilly and PetDx and has received research funding from Grail, not related to the work presented. D.R.J. is a member of the Advisory Council for Astra Zeneca and a member of the Clinical Trial Steering Committee for Merck. All other authors have no relevant competing interests to disclose.
Figures
Comment in
-
A genetic portrait of metastatic seeds in lung adenocarcinoma.Cancer Cell. 2023 May 8;41(5):828-830. doi: 10.1016/j.ccell.2023.04.004. Cancer Cell. 2023. PMID: 37160102
References
-
- Lou F, Huang J, Sima CS, Dycoco J, Rusch V, Bach PB, (2013), Patterns of recurrence and second primary lung cancer in early-stage lung cancer survivors followed with routine computed tomography surveillance, J Thorac Cardiovasc Surg, 145, 75–81; discussion 81–72, 10.1016/j.jtcvs.2012.09.030 - DOI - PubMed
-
- Watanabe K, Tsuboi M, Sakamaki K, Nishii T, Yamamoto T, Nagashima T, Ando K, Ishikawa Y, Woo T, Adachi H, Kumakiri Y, Maehara T, Nakayama H, Masuda M, (2016), Postoperative follow-up strategy based on recurrence dynamics for non-small-cell lung cancer, Eur J Cardiothorac Surg, 49, 1624–1631, 10.1093/ejcts/ezv462 - DOI - PubMed
-
- Brandt WS, Yan W, Zhou J, Tan KS, Montecalvo J, Park BJ, Adusumilli PS, Huang J, Bott MJ, Rusch VW, Molena D, Travis WD, Kris MG, Chaft JE, Jones DR, (2019), Outcomes after neoadjuvant or adjuvant chemotherapy for cT2–4N0–1 non-small cell lung cancer: A propensity-matched analysis, J Thorac Cardiovasc Surg, 157, 743–753 e743, 10.1016/j.jtcvs.2018.09.098 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
