

Non-alcoholic fatty liver disease is characterised by a reduced polyunsaturated fatty acid transport via free fatty acids and high-density lipoproteins (HDL)
- PMID: 37084865
- PMCID: PMC10176260
- DOI: 10.1016/j.molmet.2023.101728
Non-alcoholic fatty liver disease is characterised by a reduced polyunsaturated fatty acid transport via free fatty acids and high-density lipoproteins (HDL)
Abstract
Background and objectives: Non-alcoholic fatty liver disease (NAFLD) develops due to impaired hepatic lipid fluxes and is a risk factor for chronic liver disease and atherosclerosis. Lipidomic studies consistently reported characteristic hepatic/VLDL "lipid signatures" in NAFLD; whole plasma traits are more debated. Surprisingly, the HDL lipid composition by mass spectrometry has not been characterised across the NAFLD spectrum, despite HDL being a possible source of hepatic lipids delivered from peripheral tissues alongside free fatty acids (FFA). This study characterises the HDL lipidomic signature in NAFLD, and its correlation with metabolic and liver disease markers.
Methods: We used liquid chromatography-mass spectrometry to determine the whole serum and HDL lipidomic profile in 89 biopsy-proven NAFLD patients and 20 sex and age-matched controls.
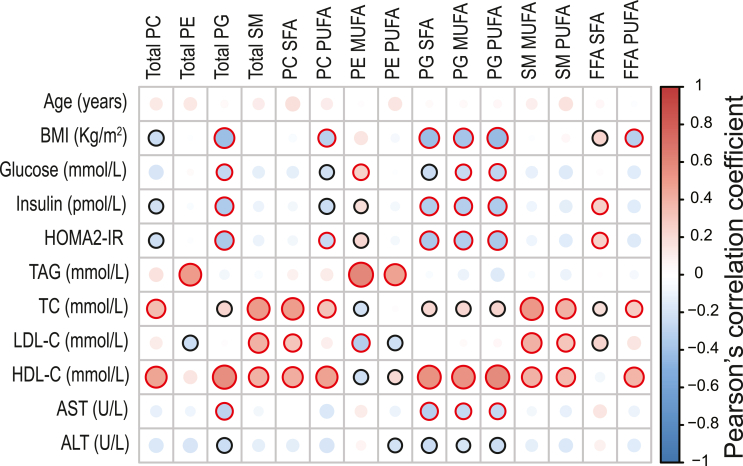
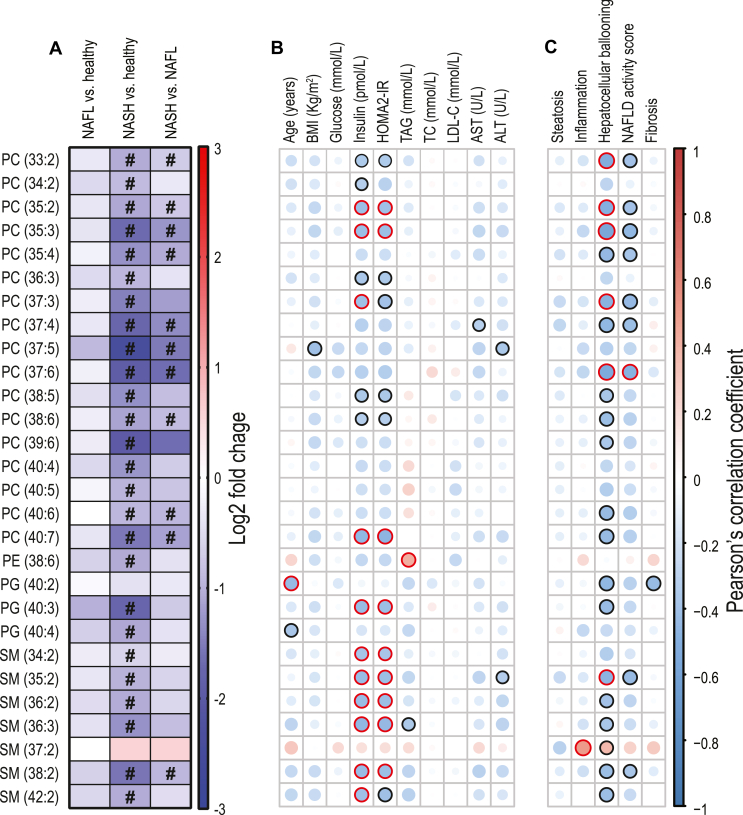
Results: In the whole serum of NAFLD versus controls, we report a depletion in polyunsaturated (PUFA) phospholipids (PL) and FFA; with PUFA PL being also lower in HDL, and negatively correlated with BMI, insulin resistance, triglycerides, and hepatocyte ballooning. In the HDL of the NAFLD group we also describe higher saturated ceramides, which positively correlate with insulin resistance and transaminases.
Conclusion: NAFLD features lower serum lipid species containing polyunsaturated fatty acids; the most affected lipid fractions are FFA and (HDL) phospholipids; our data suggest a possible defect in the transfer of PUFA from peripheral tissues to the liver in NAFLD. Mechanistic studies are required to explore the biological implications of our findings addressing if HDL composition can influence liver metabolism and damage, thus contributing to NAFLD pathophysiology.
Keywords: LC-MS; Lipidomics; Lipoprotein metabolism; Non-alcoholic fatty liver disease (NAFLD); Obesity.
Copyright © 2023 The Authors. Published by Elsevier GmbH.. All rights reserved.
Figures



References
-
- Azzu V., Vacca M., Virtue S., Allison M., Vidal-Puig A. Adipose tissue-liver cross talk in the control of whole-body metabolism: implications in nonalcoholic fatty liver disease. Gastroenterology. 2020;158(7):1899–1912. - PubMed
-
- Younossi Z., Anstee Q.M., Marietti M., Hardy T., Henry L., Eslam M., et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. - PubMed
-
- Younossi Z.M., Koenig A.B., Abdelatif D., Fazel Y., Henry L., Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. - PubMed
-
- Targher G., Byrne C.D., Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;69(9):1691–1705. - PubMed
-
- Mantovani A., Csermely A., Petracca G., Beatrice G., Corey K.E., Simon T.G., et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(11):903–913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
