

Structured physical exercise for bipolar depression: an open-label, proof-of concept study
- PMID: 37085592
- PMCID: PMC10121991
- DOI: 10.1186/s40345-023-00294-8
Structured physical exercise for bipolar depression: an open-label, proof-of concept study
Abstract
Background: Physical exercise (PE) is a recommended lifestyle intervention for different mental disorders and has shown specific positive therapeutic effects in unipolar depressive disorder. Considering the similar symptomatology of the depressive phase in patients with bipolar disorder (BD) and unipolar depressive disorder, it is reasonable to suggest that PE may also be beneficial for bipolar depression. However, there is an absence of studies evaluating the antidepressant effect of a structured PE intervention in BD.
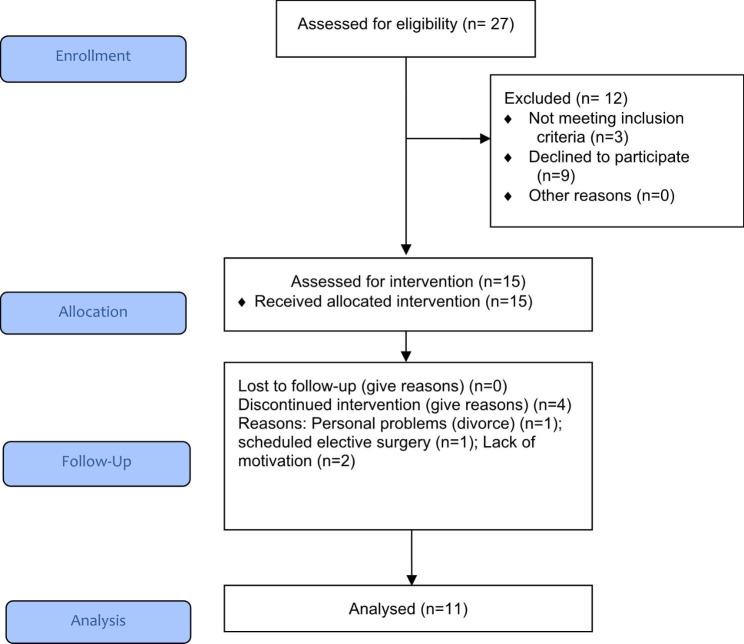
Methods: This is an open-label, single-arm study trial. Fifteen patients with a diagnosis of BD Type I or Type II, presenting a depressive episode were included in the study. After physical and functional evaluation, patients participated in supervised training sessions with aerobics followed by strength exercises, three times per week, for 12 weeks (36 training sessions). Depressive and manic symptoms were assessed at baseline and 2, 4, 8, and 12 weeks. Additionally, quality of Life and functioning were assessed at baseline and 4, 8, and 12 weeks). Finally, we tested cardiorespiratory fitness, muscle strength and body composition at baseline and week-12.
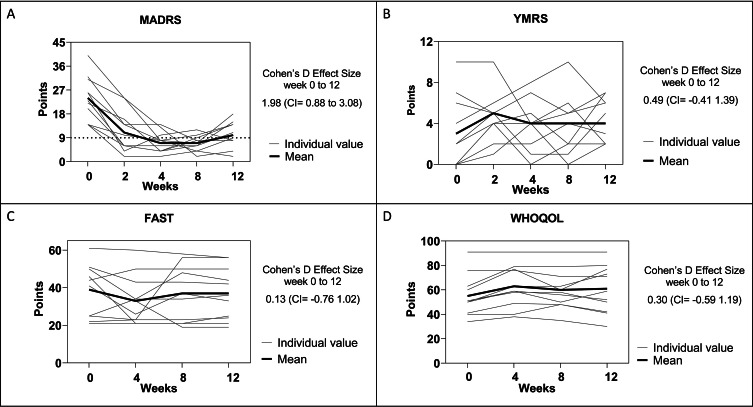
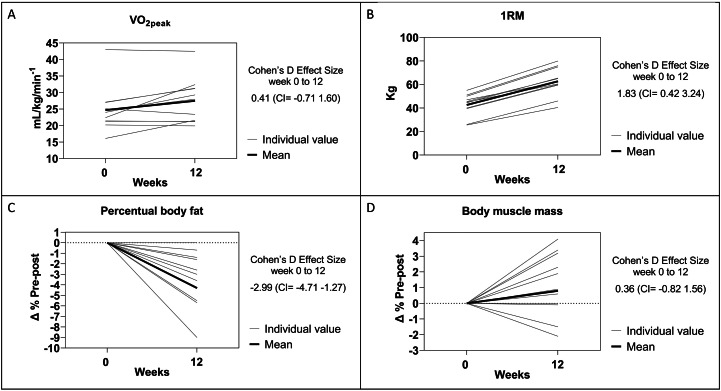
Results: The mean (± SD) Montgomery Asberg Depression Rating Scale (MADRS) score at baseline was 23.6 ± 8.3 points and after 12 weeks of PE the mean score was 10.2 ± 4.8 points. Nine patients (82%) presented an antidepressant response defined as a reduction of more than 50% of depressive symptoms at week 12 with five of those patients (45%) presenting criteria for full remission. A large and significant Cohen's D Effect Size (pre-post) was verified for MADRS reduction [1.98 (95% Confidence interval = 0.88 to 3.08)]. We did not detect a significant change in manic symptoms, functioning, and quality of life during the 12-week follow-up. At week-12, all patients increased their muscular strength (one repetition maximal test - 1RM) and reduced the percentage of body fat (spectral bioelectrical impedance analysis).
Conclusions: This study, using rigorous criteria and a structured intervention, provides valid pilot data, showing the feasibility of a structured PE intervention for the treatment of depressive symptoms in BD, and suggesting a potential adjunctive antidepressant effect. Moreover, PE showed a positive impact on muscle strength and body composition. This should be further verified by randomized controlled studies.
Keywords: Bipolar disorder; Depression; Mental health; Physical activity; Physical exercise.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Brown LE, Weir JP. ASEP procedures recommendation I: accurate assessment of muscular strength and power. J Exerc Physiol Online. 2001.
LinkOut - more resources
Full Text Sources
