

Technical development and validation of a clinically applicable microenvironment classifier as a biomarker of tumour hypoxia for soft tissue sarcoma
- PMID: 37085598
- PMCID: PMC10241814
- DOI: 10.1038/s41416-023-02265-3
Technical development and validation of a clinically applicable microenvironment classifier as a biomarker of tumour hypoxia for soft tissue sarcoma
Abstract
Background: Soft tissue sarcomas (STS) are rare, heterogeneous tumours and biomarkers are needed to inform management. We previously derived a prognostic tumour microenvironment classifier (24-gene hypoxia signature). Here, we developed/validated an assay for clinical application.
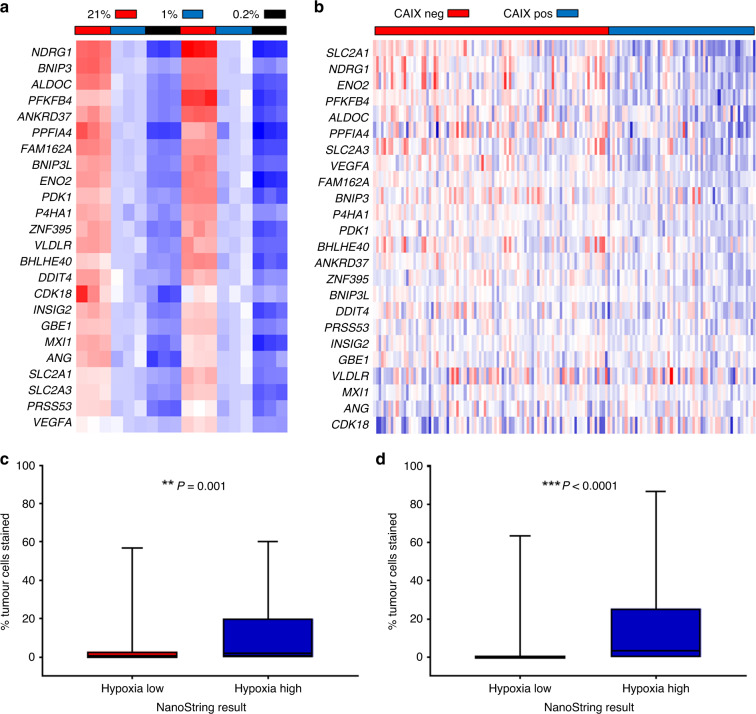
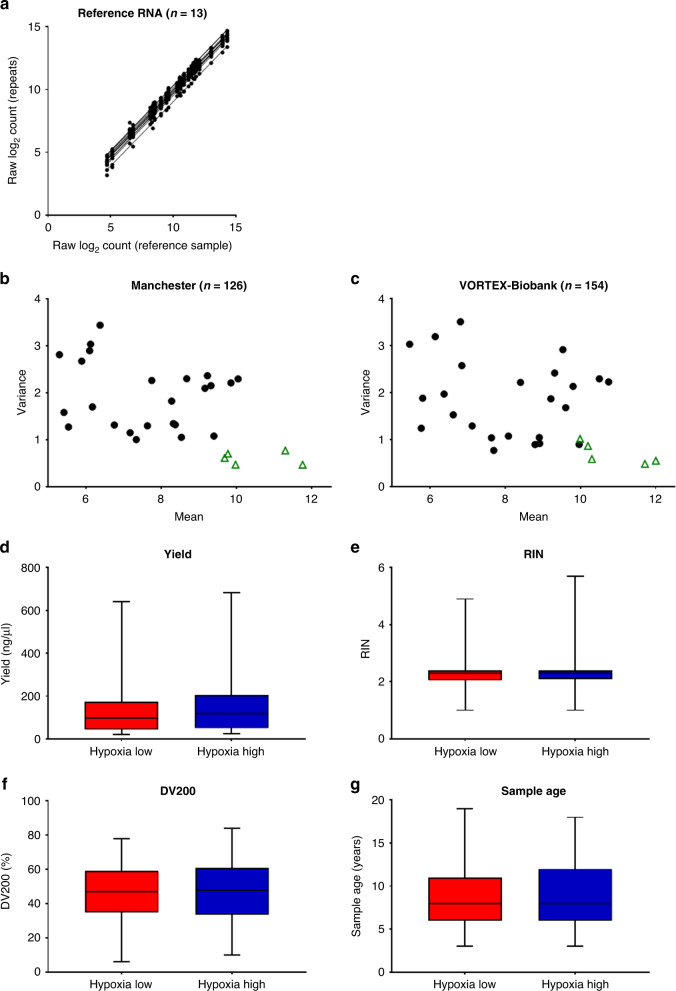
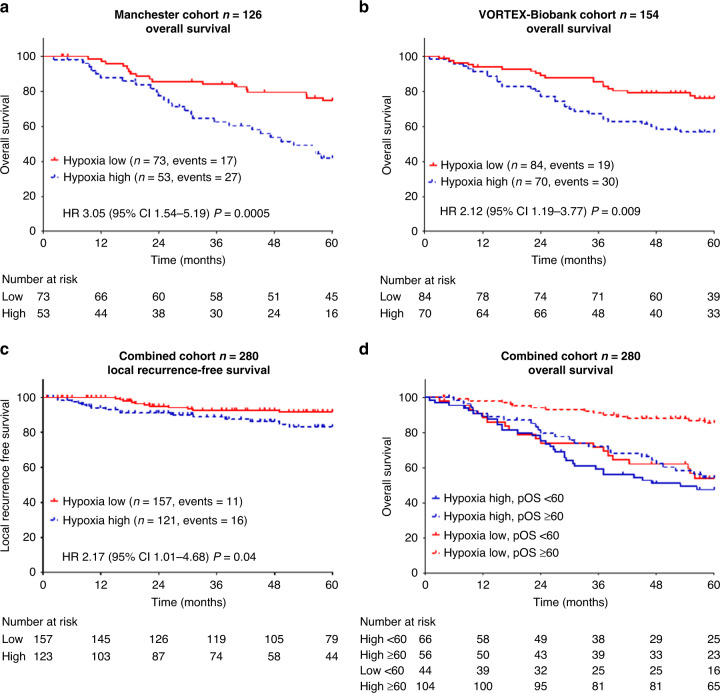
Methods: Technical performance of targeted assays (Taqman low-density array, nanoString) was compared in 28 prospectively collected formalin-fixed, paraffin-embedded (FFPE) biopsies. The nanoString assay was biologically validated by comparing to HIF-1α/CAIX immunohistochemistry (IHC) in clinical samples. The Manchester (n = 165) and VORTEX Phase III trial (n = 203) cohorts were used for clinical validation. The primary outcome was overall survival (OS).
Results: Both assays demonstrated excellent reproducibility. The nanoString assay detected upregulation of the 24-gene signature under hypoxia in vitro, and 16/24 hypoxia genes were upregulated in tumours with high CAIX expression in vivo. Patients with hypoxia-high tumours had worse OS in the Manchester (HR 3.05, 95% CI 1.54-5.19, P = 0.0005) and VORTEX (HR 2.13, 95% CI 1.19-3.77, P = 0.009) cohorts. In the combined cohort, it was independently prognostic for OS (HR 2.24, 95% CI 1.42-3.53, P = 0.00096) and associated with worse local recurrence-free survival (HR 2.17, 95% CI 1.01-4.68, P = 0.04).
Conclusions: This study comprehensively validates a microenvironment classifier befitting FFPE STS biopsies. Future uses include: (1) selecting high-risk patients for perioperative chemotherapy; and (2) biomarker-driven trials of hypoxia-targeted therapies.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO Classification of Tumours Editorial Board: WHO Classification of Tumours of Soft Tissue and Bone, World Health Organization Classification of Tumours (ed 5th). Lyon, France, International Agency for Research on Cancer; 2020, p. 607.
-
- Tap WD, Wagner AJ, Schöffski P, Martin-Broto J, Krarup-Hansen A, Ganjoo KN, et al. Effect of doxorubicin plus olaratumab vs doxorubicin plus placebo on survival in patients with advanced soft tissue sarcomas: the ANNOUNCE randomized clinical trial. J Am Med Assoc. 2020;323:1266–76. doi: 10.1001/jama.2020.1707. - DOI - PMC - PubMed
-
- Woll PJ, Reichardt P, Le Cesne A, Bonvalot S, Azzarelli A, Hoekstra HJ, et al. Adjuvant chemotherapy with doxorubicin, ifosfamide, and lenograstim for resected soft-tissue sarcoma (EORTC 62931): a multicentre randomised controlled trial. Lancet Oncol. 2012;13:1045–54. doi: 10.1016/S1470-2045(12)70346-7. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
