

A comprehensive diagnostic approach in suspected neurosarcoidosis
- PMID: 37085608
- PMCID: PMC10121682
- DOI: 10.1038/s41598-023-33631-z
A comprehensive diagnostic approach in suspected neurosarcoidosis
Abstract
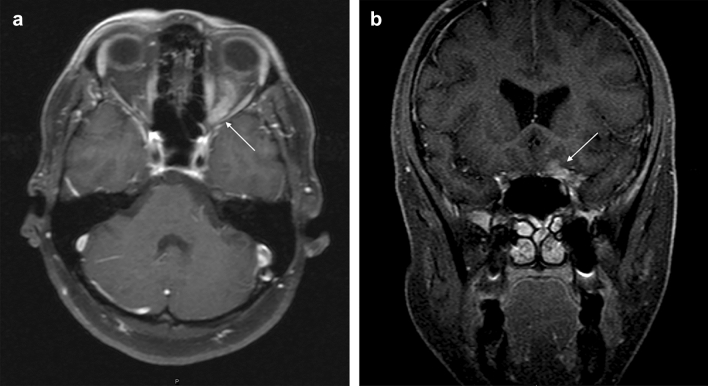
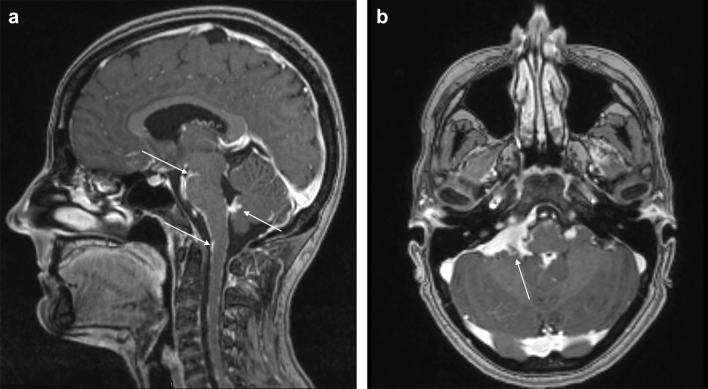
Neurosarcoidosis presents a diagnostic challenge in clinical settings, as it has no pathognomonic symptoms or signs and a wide range of differential diagnoses. The aim of this report is to present the pathological features of our group of patients, obtained through a systematic diagnostic approach. This retrospective cohort study enrolled all adult patients primarily diagnosed with neurosarcoidosis at the neurology department of a tertiary center in Sweden over a period of 30 years, from 1990 to 2021. We identified 90 patients, 54 with possible neurosarcoidosis and 36 with probable neurosarcoidosis. CNS biopsy revealed an alternative diagnosis for 24 patients, who were then excluded. The collected data from medical records included demographic and clinical characteristics, systemic and/or neurological isolated involvement, various laboratory tests, including cerebrospinal fluid (CSF), serum analysis, imaging studies (MRI, FDG-PET/CT, and HRCT), nerve conduction studies, electromyography, and pathology reports of central nervous system (CNS), and extra-neural tissue biopsies. Sixty-six patients were included in our cohort. The median age at onset of symptoms was 49 years, with a similar sex distribution. Cranial neuropathies (38%), motor deficit (32%), headache (16%), and pituitary dysfunction (12%) were the most common presenting features. CSF studies were abnormal in 77% of the patients, who showed lymphocytosis (57%), elevated protein (44%), oligoclonal bands (40%), elevated ACE (28%), and raised T lymphocyte CD4+/CD8+ ratios (13%). Strikingly, MRI showed that 17% of the patients presented with isolated pituitary gland lesions. FDG-PET/CT was performed in 22 patients (33%) and confirmed systemic sarcoidosis in 11. Despite our extensive workup, the final classification for our patients only allowed for a definite diagnosis in 14 patients; the remainder were classified as probable (32) or possible (20) neurosarcoidosis. Since 2007, the employment of a structured laboratory and imaging approach and the increasing number of CNS biopsies have facilitated and improved the process of correct attribution in patients with presumptive neurosarcoidosis, especially in patients with isolated neurological lesions. We highlight a higher frequency of pituitary lesions due to neurosarcoidosis than has been classically described. A detailed laboratory diagnostic workup is included.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
