

The right ventricular dysfunction and ventricular interdependence in patients with DM: assessment using cardiac MR feature tracking
- PMID: 37085847
- PMCID: PMC10122304
- DOI: 10.1186/s12933-023-01806-7
The right ventricular dysfunction and ventricular interdependence in patients with DM: assessment using cardiac MR feature tracking
Abstract
Background: To investigate the difference of right ventricular (RV) structural and functional alteration in patients with diabetes mellitus (DM) with preserved left ventricular ejection fraction (LVEF), and the ventricular interdependence in these patients, using cardiac MR (CMR) feature tracking.
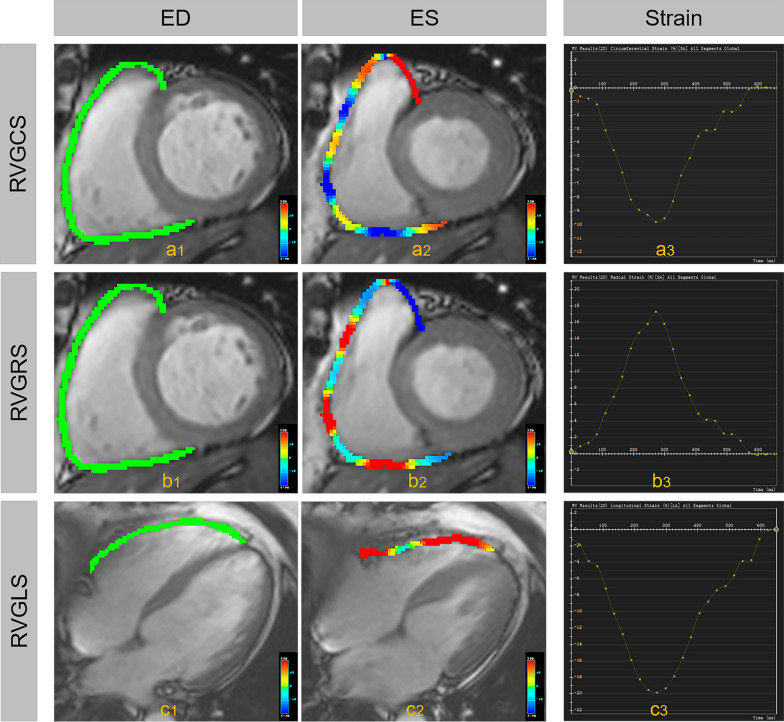
Methods: From December 2016 to February 2022, 148 clinically diagnosed patients with DM who underwent cardiac MR (CMR) in our hospital were consecutively recruited. Fifty-four healthy individuals were included as normal controls. Biventricular strains, including left/right ventricular global longitudinal strain (LV-/RVGLS), left/right ventricular global circumferential strain (LV-/RVGCS), left/right ventricular global radial strain (LV-/RVGRS) were evaluated, and compared between patients with DM and healthy controls. Multiple linear regression and mediation analyses were used to evaluate DM's direct and indirect effects on RV strains.
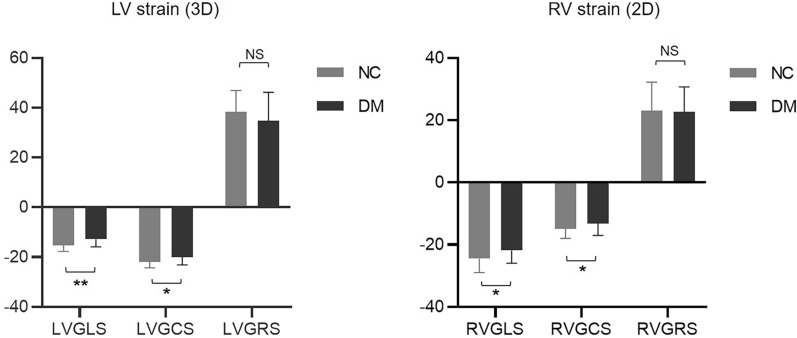
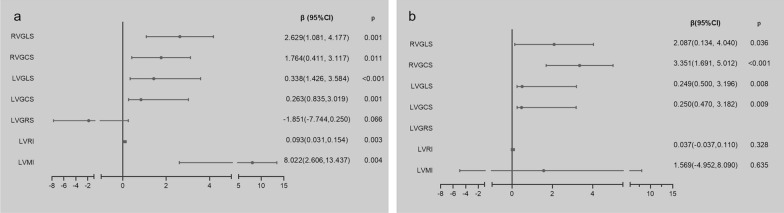
Results: No differences were found in age (56.98 ± 10.98 vs. 57.37 ± 8.41, p = 0.985), sex (53.4% vs. 48.1%, p = 0.715), and body surface area (BSA) (1.70 ± 0.21 vs. 1.69 ± 0.17, p = 0.472) between DM and normal controls. Patients with DM had decreased RVGLS (- 21.86 ± 4.14 vs. - 24.49 ± 4.47, p = 0.001), RVGCS (- 13.16 ± 3.86 vs. - 14.92 ± 3.08, p = 0.011), and no decrease was found in RVGRS (22.62 ± 8.11 vs. 23.15 ± 9.05, p = 0.743) in patients with DM compared with normal controls. The difference in RVGLS between normal controls and patients with DM was totally mediated by LVGLS (indirect effecting: 0.655, bootstrapped 95%CI 0.138-0.265). The difference in RVGCS between normal controls and DM was partly mediated by the LVGLS (indirect effecting: 0.336, bootstrapped 95%CI 0.002-0.820) and LVGCS (indirect effecting: 0.368, bootstrapped 95%CI 0.028-0.855).
Conclusions: In the patients with DM and preserved LVEF, the difference in RVGLS between DM and normal controls was totally mediated by LVGLS. Although there were partly mediating effects of LVGLS and LVGCS, the decrease in RVGCS might be directly affected by the DM.
Keywords: CMR feature-tracking; Diabetes mellitus; Right ventricular dysfunction; Ventricular interdependence.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Impact of diabetes mellitus on right ventricular dysfunction and ventricular interdependence in hypertensive patients with heart failure with reduced ejection fraction assessed via 3.0 T cardiac MRI.Cardiovasc Diabetol. 2024 Oct 23;23(1):375. doi: 10.1186/s12933-024-02472-z. Cardiovasc Diabetol. 2024. PMID: 39443983 Free PMC article.
-
Subclinical systolic dysfunction detected by 2D speckle tracking echocardiography in adults with diabetes mellitus: systematic review and meta-analysis of 6668 individuals with diabetes mellitus and 7218 controls.Int J Cardiovasc Imaging. 2023 May;39(5):977-989. doi: 10.1007/s10554-023-02810-4. Epub 2023 Mar 30. Int J Cardiovasc Imaging. 2023. PMID: 36995526 Free PMC article.
-
Cardiovascular magnetic resonance-derived myocardial strain in asymptomatic heart transplanted patients and its correlation with late gadolinium enhancement.Eur Radiol. 2020 Aug;30(8):4337-4346. doi: 10.1007/s00330-020-06763-3. Epub 2020 Mar 31. Eur Radiol. 2020. PMID: 32232791
-
Biventricular Dysfunction and Ventricular Interdependence in Patients With Pulmonary Hypertension: A 3.0-T Cardiac MRI Feature Tracking Study.J Magn Reson Imaging. 2024 Jul;60(1):350-362. doi: 10.1002/jmri.29044. Epub 2023 Oct 21. J Magn Reson Imaging. 2024. PMID: 37864419
-
MRI-Derived Myocardial Strain Measures in Normal Subjects.JACC Cardiovasc Imaging. 2018 Feb;11(2 Pt 1):196-205. doi: 10.1016/j.jcmg.2016.12.025. Epub 2017 May 17. JACC Cardiovasc Imaging. 2018. PMID: 28528164
Cited by
-
Effects of diabetes mellitus and glycemic traits on cardiovascular morpho-functional phenotypes.Cardiovasc Diabetol. 2023 Dec 8;22(1):336. doi: 10.1186/s12933-023-02079-w. Cardiovasc Diabetol. 2023. PMID: 38066511 Free PMC article.
-
Impact of diabetes mellitus on right ventricular dysfunction and ventricular interdependence in hypertensive patients with heart failure with reduced ejection fraction assessed via 3.0 T cardiac MRI.Cardiovasc Diabetol. 2024 Oct 23;23(1):375. doi: 10.1186/s12933-024-02472-z. Cardiovasc Diabetol. 2024. PMID: 39443983 Free PMC article.
-
The right ventricular dysfunction and ventricular interdependence in patients with T2DM and aortic regurgitation: an assessment using CMR feature tracking.Cardiovasc Diabetol. 2024 Aug 8;23(1):294. doi: 10.1186/s12933-024-02372-2. Cardiovasc Diabetol. 2024. PMID: 39118075 Free PMC article.
-
Progress in Cardiac Magnetic Resonance Feature Tracking for Evaluating Myocardial Strain in Type-2 Diabetes Mellitus.Curr Diabetes Rev. 2024;20(8):98-109. doi: 10.2174/0115733998277127231211063107. Curr Diabetes Rev. 2024. PMID: 38310480 Free PMC article. Review.
References
-
- Disease C, Management R. Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S144–s174. - PubMed
-
- Pop-Busui R, Januzzi JL, Bruemmer D, Butalia S, Green JB, Horton WB, Knight C, Levi M, Rasouli N, Richardson CR. Heart failure: an underappreciated complication of diabetes a consensus report of the American diabetes association. Diabetes Care. 2022;45(7):1670–1690. doi: 10.2337/dci22-0014. - DOI - PMC - PubMed
-
- Prázný M, Suplotova L, Gumprecht J, Kamenov Z, Fülöp T, Medvedchikov A, Rosenzweig D, Aleksandric M. Real-world characteristics, modern antidiabetic treatment patterns, and comorbidities of patients with type 2 diabetes in central and Eastern Europe: retrospective cross-sectional and longitudinal evaluations in the CORDIALLY® study. Cardiovasc Diabetol. 2022;21(1):203. doi: 10.1186/s12933-022-01631-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
