

Incremental costs of hospital-acquired infections in COVID-19 patients in an adult intensive care unit of a tertiary hospital from a low-resource setting
- PMID: 37085906
- PMCID: PMC10120483
- DOI: 10.1186/s13756-023-01240-0
Incremental costs of hospital-acquired infections in COVID-19 patients in an adult intensive care unit of a tertiary hospital from a low-resource setting
Abstract
Background: Hospital-acquired infections (HAIs) are a global public health problem and put patients at risk of complications, including death. HAIs increase treatment costs, but their financial impact on Serbia's healthcare system is unknown. Our goal was to assess incremental costs of HAIs in a tertiary care adult intensive care unit (ICU) that managed COVID-19 patients.
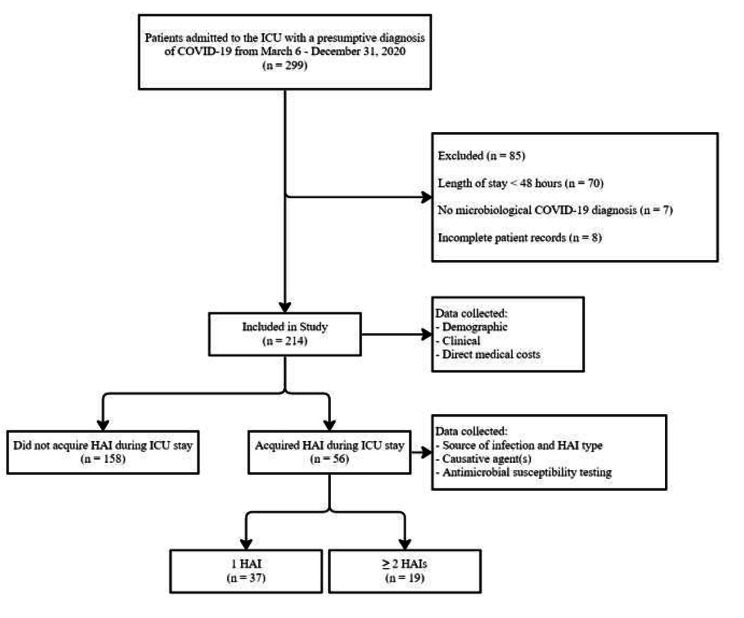
Methods: A retrospective study from March 6th to December 31st, 2020 included patients with microbiologically confirmed COVID-19 (positive rapid antigen test or real-time polymerase chain reaction) treated in the ICU of the Teaching Hospital for Infectious and Tropical Diseases, University Clinical Centre of Serbia. Demographic and HAI-specific data acquired in our ICU were collected, including total and stratified medical costs (services, materials, laboratory testing, medicines, occupancy costs). Median total and stratified costs were compared in relation to HAI acquisition. Linear regression modelling was used to assess incremental costs of HAIs, adjusted for age, biological sex, prior hospitalisation, Charlson Comorbidity Index (CCI), and Glasgow Coma Scale (GCS) on admission. Outcome variables were length of stay (LOS) in days and mortality.
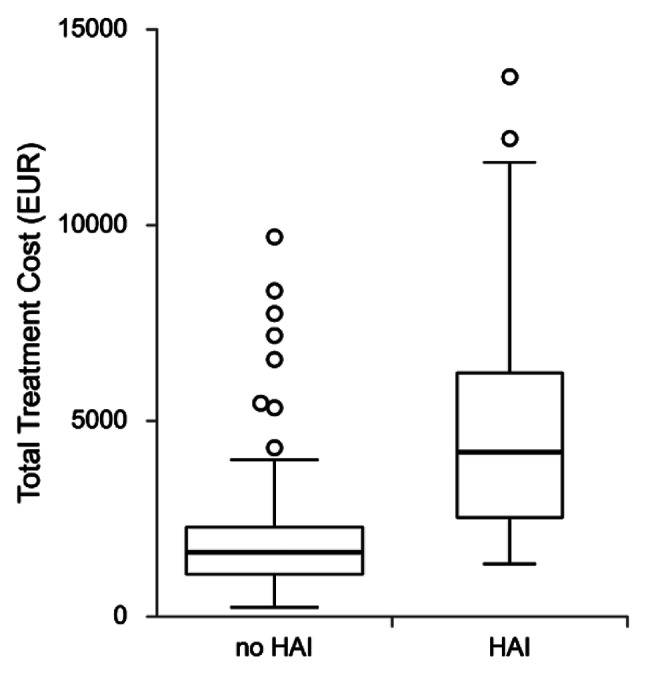
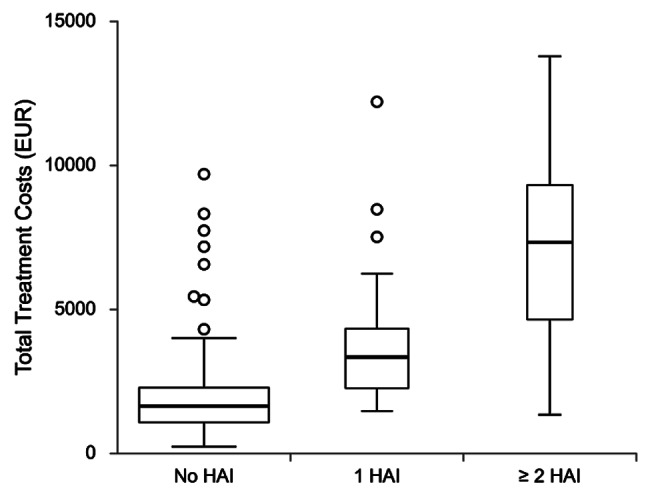
Results: During the study period, 299 patients were treated for COVID-19, of which 214 were included. HAIs were diagnosed in 56 (26.2%) patients. Acinetobacter spp. was the main pathogen in respiratory (38, 45.8%) and bloodstream infections (35, 42.2%), the two main HAI types. Median total costs were significantly greater in patients with HAIs (€1650.4 vs. €4203.2, p < 0.001). Longer LOS (10.0 vs. 18.5 days, p < 0.001) and higher ICU mortality (51.3% vs. 89.3%, p < 0.001) were seen if HAIs were acquired. Patients with ≥ 2 HAIs had the highest median total costs compared to those without HAIs or with a single HAI (€1650.4 vs. €3343.4 vs. €7336.9, p < 0.001). Incremental costs in patients with 1 and ≥ 2 HAIs were €1837.8 (95% CI 1257.8-2417.7, p < 0.001) and €5142.5 (95% CI 4262.3-6022.7, p < 0.001), respectively.
Conclusions: This is the first economic evaluation of HAIs in Serbia, showing significant additional costs to our healthcare system. HAIs prolong LOS and influence ICU mortality rates. Larger economic assessments are needed to enhance infection control practices.
Keywords: COVID-19; Economic evaluation; Hospital-acquired infections; Intensive care unit; Medical costs; Serbia.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Increased financial burdens and lengths of stay in patients with healthcare-associated infections due to multidrug-resistant bacteria in intensive care units: A propensity-matched case-control study.PLoS One. 2020 May 18;15(5):e0233265. doi: 10.1371/journal.pone.0233265. eCollection 2020. PLoS One. 2020. PMID: 32421700 Free PMC article.
-
Patient-level cost analysis of intensive care unit-acquired infections: a prospective cohort study.J Hosp Infect. 2025 May;159:106-114. doi: 10.1016/j.jhin.2024.07.002. Epub 2024 Jul 18. J Hosp Infect. 2025. PMID: 39032569
-
Costs of healthcare-associated infections to the Brazilian public Unified Health System in a tertiary-care teaching hospital: a matched case-control study.J Hosp Infect. 2020 Oct;106(2):303-310. doi: 10.1016/j.jhin.2020.07.015. Epub 2020 Jul 18. J Hosp Infect. 2020. PMID: 32693085
-
Hospital acquired COVID-19 infections amongst patients before the rollout of COVID-19 vaccinations, a scoping review.BMC Infect Dis. 2022 Feb 10;22(1):140. doi: 10.1186/s12879-022-07128-5. BMC Infect Dis. 2022. PMID: 35144556 Free PMC article.
-
Does copper treatment of commonly touched surfaces reduce healthcare-acquired infections? A systematic review and meta-analysis.J Hosp Infect. 2020 Dec;106(4):765-773. doi: 10.1016/j.jhin.2020.09.005. Epub 2020 Sep 9. J Hosp Infect. 2020. PMID: 32916212 Free PMC article.
Cited by
-
Artificial intelligence in hospital infection prevention: an integrative review.Front Public Health. 2025 Apr 2;13:1547450. doi: 10.3389/fpubh.2025.1547450. eCollection 2025. Front Public Health. 2025. PMID: 40241963 Free PMC article. Review.
References
-
- Suetens C, Latour K, Kärki T, Ricchizzi E, Kinross P, Moro ML et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017.Euro Surveill. 2018;23(46). - PMC - PubMed
-
- Cassini A, Högberg LD, Plachouras D, Quattrocchi A, Hoxha A, Simonsen GS, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66. doi: 10.1016/S1473-3099(18)30605-4. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
