

Association between the timing of ICU admission and mortality in patients with hospital-onset sepsis: a nationwide prospective cohort study
- PMID: 37085923
- PMCID: PMC10120484
- DOI: 10.1186/s40560-023-00663-6
Association between the timing of ICU admission and mortality in patients with hospital-onset sepsis: a nationwide prospective cohort study
Abstract
Background: Based on sparse evidence, the current Surviving Sepsis Campaign guideline suggests that critically ill patients with sepsis be admitted to the intensive care unit (ICU) within 6 h. However, limited ICU bed availability often makes immediate transfer difficult, and it is unclear whether all patients will benefit from early admission to the ICU. Therefore, the purpose of this study was to determine the association between the timing of ICU admission and mortality in patients with hospital-onset sepsis.
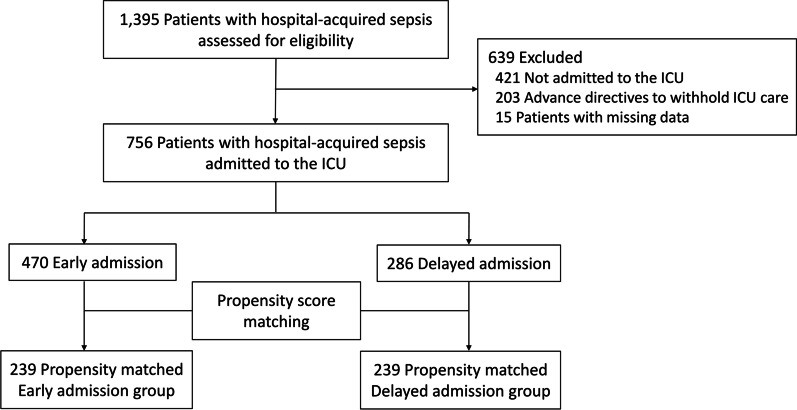
Methods: This nationwide prospective cohort study analyzed patients with hospital-onset sepsis admitted to the ICUs of 19 tertiary hospitals between September 2019 and December 2020. ICU admission was classified as either early (within 6 h) or delayed (beyond 6 h). The primary outcome of in-hospital mortality was compared using logistic regression adjusted for key prognostic factors in the unmatched and 1:1 propensity-score-matched cohorts. Subgroup and interaction analyses assessed whether in-hospital mortality varied according to baseline characteristics.
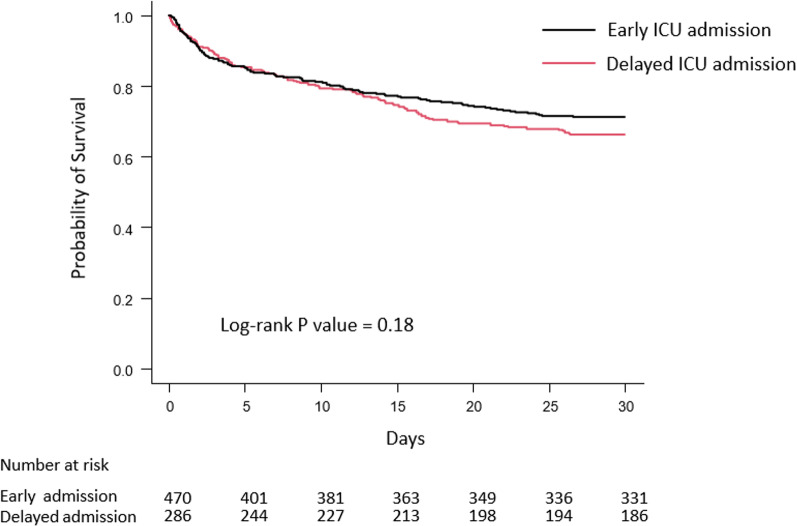
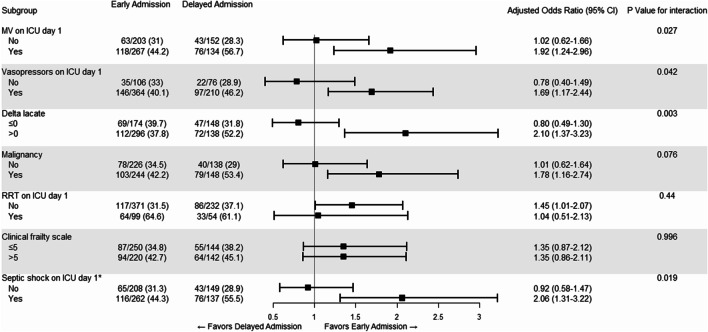
Results: A total of 470 and 286 patients were included in the early and delayed admission groups, respectively. Early admission to the ICU did not significantly result in lower in-hospital mortality in both the unmatched (adjusted odds ratio [aOR], 1.35; 95% confidence interval [CI], 0.99-1.85) and matched cohorts (aOR, 1.38; 95% CI, 0.94-2.02). Subgroup analyses showed that patients with increasing lactate levels (aOR, 2.10; 95% CI, 1.37-3.23; P for interaction = 0.003), septic shock (aOR, 2.06; 95% CI, 1.31-3.22; P for interaction = 0.019), and those who needed mechanical ventilation (aOR, 1.92; 95% CI, 1.24-2.96; P for interaction = 0.027) or vasopressor support (aOR, 1.69; 95% CI, 1.17-2.44; P for interaction = 0.042) on the day of ICU admission had a higher risk of mortality with delayed admission.
Conclusions: Among patients with hospital-onset sepsis, in-hospital mortality did not differ significantly between those with early and delayed ICU admission. However, as early intensive care may benefit those with increasing lactate levels, septic shock, and those who require vasopressors or ventilatory support, admission to the ICU within 6 h should be considered for these subsets of patients.
Keywords: Intensive care unit; Patient admission; Prognosis; Sepsis; Septic shock; Transfer.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Prognostic factors in critically ill cancer patients admitted to the intensive care unit.J Crit Care. 2014 Aug;29(4):618-26. doi: 10.1016/j.jcrc.2014.01.014. Epub 2014 Jan 29. J Crit Care. 2014. PMID: 24612762
-
Association between statin therapy and outcomes in critically ill patients: a nested cohort study.BMC Clin Pharmacol. 2011 Aug 6;11:12. doi: 10.1186/1472-6904-11-12. BMC Clin Pharmacol. 2011. PMID: 21819615 Free PMC article. Clinical Trial.
-
Delta Shock Index During Emergency Department Stay Is Associated With in Hospital Mortality in Critically Ill Patients.Front Med (Lausanne). 2021 Apr 22;8:648375. doi: 10.3389/fmed.2021.648375. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33968957 Free PMC article.
-
Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: a systematic review and meta-analysis.Crit Care. 2016 Jun 15;20(1):181. doi: 10.1186/s13054-016-1360-z. Crit Care. 2016. PMID: 27306751 Free PMC article.
-
Impact of common comorbidities on antimicrobial consumption and mortality amongst critically ill COVID-19 patients: A retrospective two center study in Saudi Arabia.Clin Infect Pract. 2023 Jul;19:100229. doi: 10.1016/j.clinpr.2023.100229. Epub 2023 May 4. Clin Infect Pract. 2023. PMID: 37168925 Free PMC article. Review.
Cited by
-
Point-of-Care Serum Proenkephalin as an Early Predictor of Mortality in Patients Presenting to the Emergency Department with Septic Shock.Biomedicines. 2024 May 2;12(5):1004. doi: 10.3390/biomedicines12051004. Biomedicines. 2024. PMID: 38790966 Free PMC article.
-
Predicting responsiveness to fixed-dose methylene blue in adult patients with septic shock using interpretable machine learning: a retrospective study.Sci Rep. 2025 Mar 1;15(1):7254. doi: 10.1038/s41598-025-89934-w. Sci Rep. 2025. PMID: 40021734 Free PMC article.
-
Improving acute care outcome in internal medicine: the role of early stabilization and intermediate care unit.Intern Emerg Med. 2025 Mar;20(2):453-461. doi: 10.1007/s11739-024-03820-3. Epub 2024 Nov 21. Intern Emerg Med. 2025. PMID: 39572486
-
Impact of the timing of invasive mechanical ventilation in patients with sepsis: a multicenter cohort study.Crit Care. 2024 Sep 9;28(1):297. doi: 10.1186/s13054-024-05064-1. Crit Care. 2024. PMID: 39252133 Free PMC article.
-
Risk factors for in-hospital mortality in surgical patients with abdominal sepsis in China: a nested case-control study.BMJ Open. 2025 Apr 25;15(4):e092310. doi: 10.1136/bmjopen-2024-092310. BMJ Open. 2025. PMID: 40280608 Free PMC article.
References
-
- Prest J, Sathananthan M, Jeganathan N. Current trends in sepsis-related mortality in the United States. Crit Care Med. 2021;49(8):1276–1284. - PubMed
-
- Driessen RGH, Heijnen NFL, Hulsewe R, Holtkamp JWM, Winkens B, van de Poll MCG, et al. Early ICU-mortality in sepsis—causes, influencing factors and variability in clinical judgement: a retrospective cohort study. Infect Dis (Lond) 2021;53(1):61–68. doi: 10.1080/23744235.2020.1821912. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
