

Activation of telomerase by TA-65 enhances immunity and reduces inflammation post myocardial infarction
- PMID: 37086366
- PMCID: PMC10122201
- DOI: 10.1007/s11357-023-00794-6
Activation of telomerase by TA-65 enhances immunity and reduces inflammation post myocardial infarction
Abstract
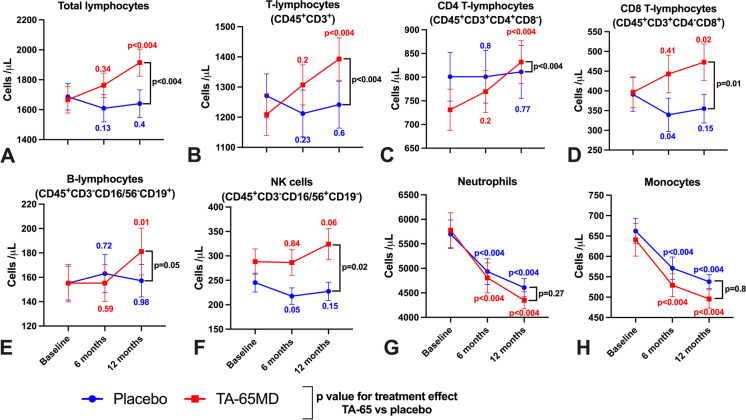
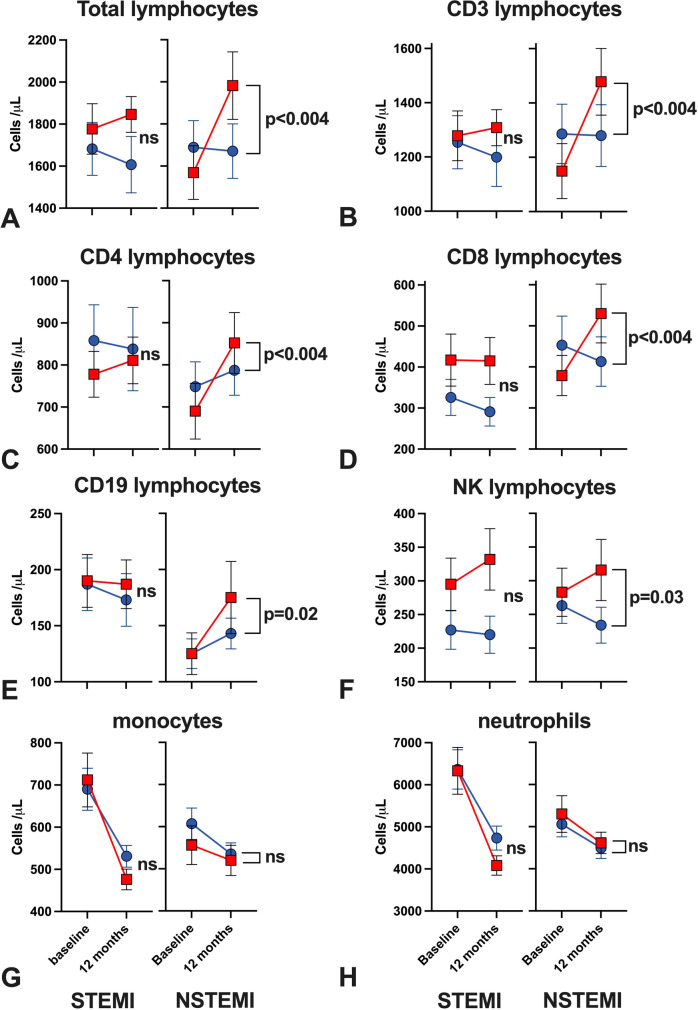
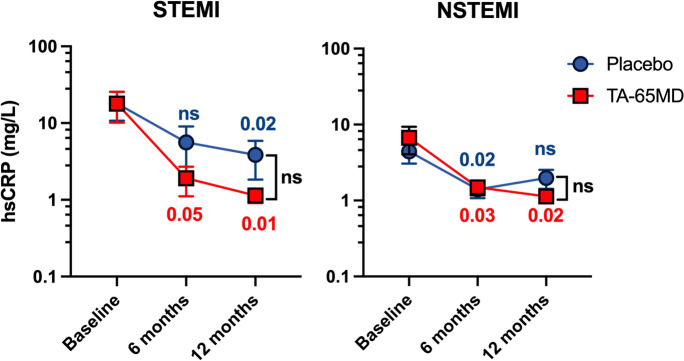
Myocardial infarction (MI) accelerates immune ageing characterised by lymphopenia, expansion of terminally differentiated CD8+ T-lymphocytes (CD8+ TEMRA) and inflammation. Pre-clinical data showed that TA-65, an oral telomerase activator, reduced immune ageing and inflammation after MI. We conducted a double blinded randomised controlled pilot trial evaluating the use of TA-65 to reduce immune cell ageing in patients following MI. Ninety MI patients aged over 65 years were randomised to either TA-65 (16 mg daily) or placebo for 12 months. Peripheral blood leucocytes were analysed by flow cytometry. The pre-defined primary endpoint was the proportion of CD8+ T-lymphocytes which were CD8+ TEMRA after 12 months. Secondary outcomes included high-sensitivity C-reactive protein (hsCRP) levels. Median age of participants was 71 years. Proportions of CD8+ TEMRA did not differ after 12 months between treatment groups. There was a significant increase in mean total lymphocyte count in the TA-65 group after 12 months (estimated treatment effect: + 285 cells/μl (95% CI: 117-452 cells/ μ l, p < 0.004), driven by significant increases from baseline in CD3+, CD4+, and CD8+ T-lymphocytes, B-lymphocytes and natural killer cells. No increase in lymphocyte populations was seen in the placebo group. At 12 months, hsCRP was 62% lower in the TA-65 group compared to placebo (1.1 vs. 2.9 mg/L). Patients in the TA-65 arm experienced significantly fewer adverse events (130 vs. 185, p = 0.002). TA-65 did not alter CD8+ TEMRA but increased all major lymphocyte subsets and reduced hsCRP in elderly patients with MI after 12 months.
Keywords: Acute myocardial infarction; Ageing; Immunosenescence; T-lymphocytes; Telomerase.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Coelho-Lima J, Georgiopoulos G, Ahmed J, Adil SER, Gaskin D, Bakogiannis C, et al. Prognostic value of admission high-sensitivity troponin in patients with ST-elevation myocardial infarction. Heart. 2021;107:1881–8. - PubMed
-
- Stamatelopoulos K, Mueller-Hennessen M, Georgiopoulos G, Sachse M, Boeddinghaus J, Sopova K, Gatsiou A, Amrhein C, Biener M, Vafaie M, Athanasouli F, Stakos D, Pateras K, Twerenbold R, Badertscher P, Nestelberger T, Dimmeler S, Katus HA, Zeiher AM, Mueller C, Giannitsis E, Stellos K. Amyloid-β (1–40) and Mortality in Patients With Non-ST-Segment Elevation Acute Coronary Syndrome: A Cohort Study. Ann Intern Med. 2018;168:855–865. doi: 10.7326/M17-1540. - DOI - PubMed
-
- Spray L, Park C, Cormack S, Mohammed A, Panahi P, Boag S, Bennaceur K, Sopova K, Richardson G, Stangl VM, Rech L, Rainer PP, Ramos GC, Hofmann U, Stellos K, Spyridopoulos I. The Fractalkine Receptor CX3CR1 Links Lymphocyte Kinetics in CMV-Seropositive Patients and Acute Myocardial Infarction With Adverse Left Ventricular Remodeling. Front Immunol. 2021;12:605857. doi: 10.3389/fimmu.2021.605857. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
