

High incidence of type 2 endoleak and low associated adverse events in the Vascular Quality Initiative linked to Medicare claims
- PMID: 37086823
- PMCID: PMC10524631
- DOI: 10.1016/j.jvs.2023.04.013
High incidence of type 2 endoleak and low associated adverse events in the Vascular Quality Initiative linked to Medicare claims
Abstract
Introduction: Type 2 endoleak (T2EL) is the most common adverse finding on postoperative surveillance after endovascular aortic aneurysm repair (EVAR). A low rate of aneurysm-related mortality with T2EL has been established. However, the optimal management strategy and the efficacy of reintervention remain controversial. This study used data from the Vascular Quality Initiative linked to Medicare claims (VQI-Medicare) to evaluate T2LE in a real-world cohort.
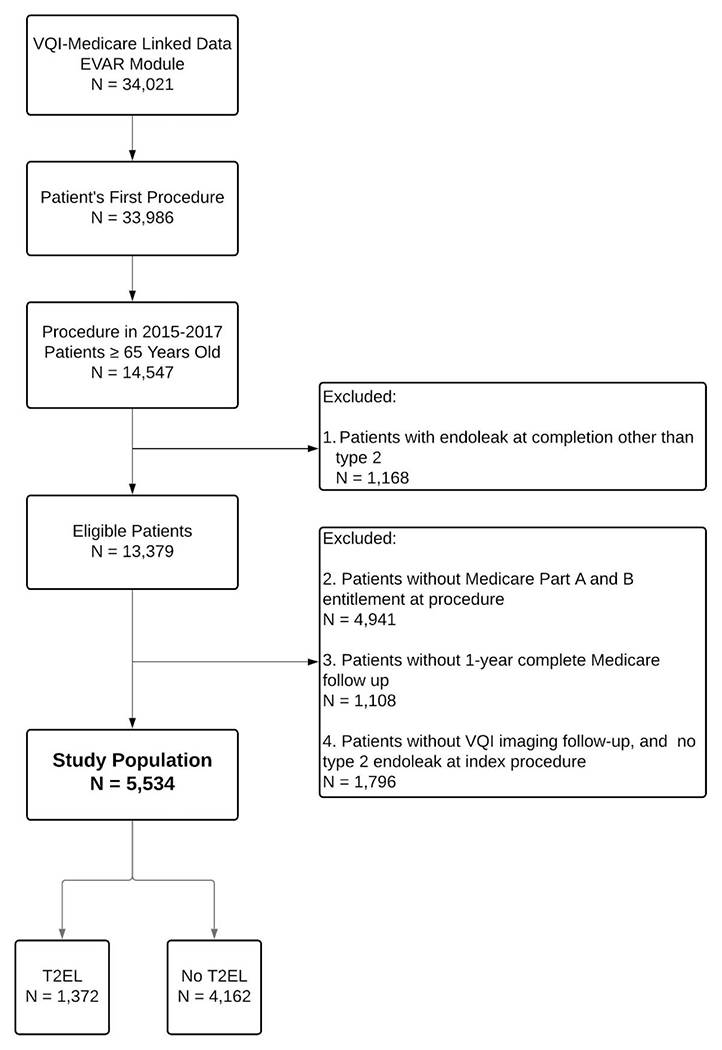
Methods: This retrospective review of EVAR procedures in VQI-Medicare included patients undergoing their first EVAR procedure between 2015 and 2017. Patients with an endoleak other than T2EL on completion angiogram and those without VQI imaging follow-up were excluded. Patients without Medicare part A or part B enrollment at the time of the procedure or without 1-year complete Medicare follow-up data were also excluded. The exposure variable was T2EL, defined as any branch vessel flow detected within the first postoperative year. Outcomes of interest were mortality, reintervention, T2EL-related reintervention, post-EVAR imaging, and T2EL behavior including spontaneous resolution, aneurysm sac regression, and resolution after reintervention. The association of prophylactic branch vessel embolization (PBE) with T2EL resolution and aneurysm sac regression was also evaluated.
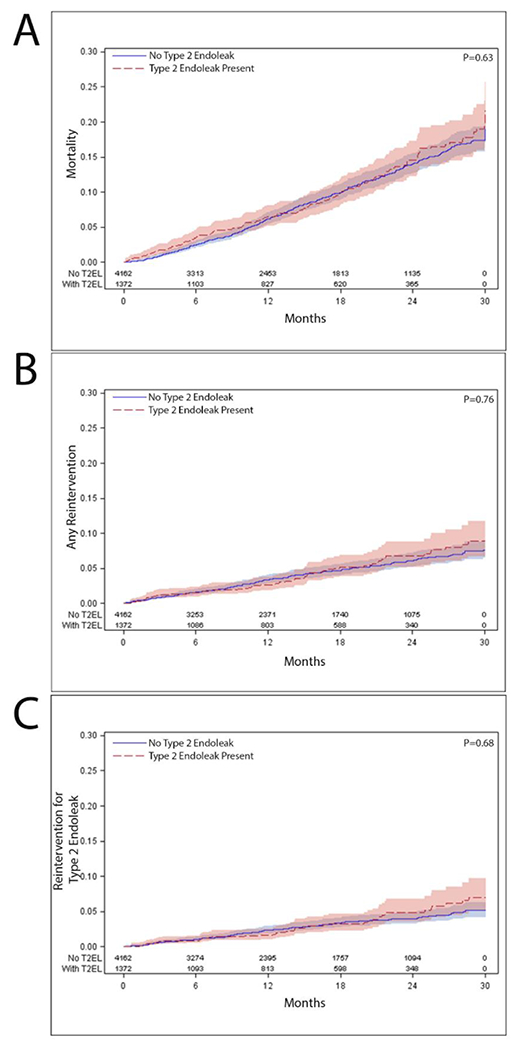
Results: In a final cohort of 5534 patients, 1372 (24.7%) had an identified T2EL and 4162 (75.2%) did not. The median age of patients with and without T2EL was 77 and 75 years, respectively. There were no differences in mortality, imaging, reintervention, or T2EL-related reintervention at 3 years after the procedure for patients with T2EL. The aneurysm sac diameter decreased by 4 mm (range: 9-0 mm decrease) in the total cohort. Patients with inferior mesenteric artery-based T2EL had the smallest decrease in aneurysm diameter (median 1 mm decrease compared with 1.5 mm for accessory renal artery-based T2EL, 2 mm for multiple feeding vessel-based T2EL, and 4 mm for lumbar artery-based T2EL; P < .001). Spontaneous resolution occurred in 73.7% of patients (n = 809). T2ELs with evidence of multiple feeding vessels were associated with the lowest rate of spontaneous resolution (n = 51, 54.9%), compared with those with a single identified feeding vessel of inferior mesenteric artery (n = 99, 60.0%), lumbar artery (n = 655, 77.7%), or accessory renal artery (n = 31, 79.5%) (P < .001). PBE was performed in 84 patients. Patients who underwent PBE and were without detectable T2EL after EVAR had the greatest rate of sac regression at follow-up (7 mm decrease) compared with baseline.
Conclusions: T2EL after EVAR is associated with high rates of spontaneous resolution, low rates of aneurysm sac growth, and no evidence of increased early mortality or reintervention. PBE in conjunction with EVAR may be indicated in some circumstances.
Keywords: Abdominal aortic aneurysm; Endoleak; Endovascular; Minimally invasive therapy.
Published by Elsevier Inc.
Figures
Similar articles
-
Outcomes associated with type II endoleaks after infrarenal endovascular aneurysm repair in the Vascular Quality Initiative linked to Medicare claims.J Vasc Surg. 2025 Sep;82(3):810-818.e5. doi: 10.1016/j.jvs.2025.04.061. Epub 2025 May 6. J Vasc Surg. 2025. PMID: 40339998
-
Surgical treatment patterns and clinical outcomes of patients treated for expanding aneurysm sacs with type II endoleaks after endovascular aneurysm repair.J Vasc Surg. 2021 Feb;73(2):484-493. doi: 10.1016/j.jvs.2020.05.062. Epub 2020 Jun 29. J Vasc Surg. 2021. PMID: 32615284
-
Relevance of Type II Endoleak After Endovascular Repair of Ruptured Abdominal Aortic Aneurysms: A Retrospective Single-Center Cohort Study.J Endovasc Ther. 2023 Aug;30(4):540-549. doi: 10.1177/15266028221086476. Epub 2022 Mar 30. J Endovasc Ther. 2023. PMID: 35352969 Free PMC article.
-
Natural History, Diagnosis, and Management of Type II Endoleaks after Endovascular Aortic Repair: Review and Update.Ann Vasc Surg. 2020 Jan;62:420-431. doi: 10.1016/j.avsg.2019.04.048. Epub 2019 Jul 31. Ann Vasc Surg. 2020. PMID: 31376537 Review.
-
An updated systematic review and meta-analysis of pre-emptive aortic side branch embolization to prevent type II endoleaks after endovascular aneurysm repair.J Vasc Surg. 2023 Jun;77(6):1815-1821. doi: 10.1016/j.jvs.2022.11.042. Epub 2022 Nov 15. J Vasc Surg. 2023. PMID: 36400361
Cited by
-
Clinical Imaging and Innovations in Aortic Aneurysm and Dissection.Semin Intervent Radiol. 2024 Dec 9;41(6):536-546. doi: 10.1055/s-0044-1800823. eCollection 2024 Dec. Semin Intervent Radiol. 2024. PMID: 40190769 Review.
-
Outcomes associated with type II endoleaks after infrarenal endovascular aneurysm repair in the Vascular Quality Initiative linked to Medicare claims.J Vasc Surg. 2025 Sep;82(3):810-818.e5. doi: 10.1016/j.jvs.2025.04.061. Epub 2025 May 6. J Vasc Surg. 2025. PMID: 40339998
References
-
- Kumar L, Cowled P, Boult M, Howell S, Fitridge R. Type II Endoleak after Endovascular Aneurysm Repair: Natural History and Treatment Outcomes. Annals of vascular surgery. 2017;44:94–102. - PubMed
-
- Dijkstra ML, Zeebregts CJ, Verhagen HJM, Teijink JAW, Power AH, Bockler D, et al. Incidence, natural course, and outcome of type II endoleaks in infrarenal endovascular aneurysm repair based on the ENGAGE registry data. Journal of vascular surgery. 2020;71(3):780–9. - PubMed
-
- Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG, participants Et. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 2004;364(9437):843–8. - PubMed
-
- United Kingdom ETI, Greenhalgh RM, Brown LC, Powell JT, Thompson SG, Epstein D, et al. Endovascular versus open repair of abdominal aortic aneurysm. The New England journal of medicine. 2010;362(20):1863–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
