

Prognostic significance of lymphovascular invasion in patients with pT1b esophageal squamous cell carcinoma
- PMID: 37087442
- PMCID: PMC10122816
- DOI: 10.1186/s12885-023-10858-7
Prognostic significance of lymphovascular invasion in patients with pT1b esophageal squamous cell carcinoma
Abstract
Background: Lymphovascular invasion (LVI) is a crucial predictor of lymph node metastasis (LNM). However, few studies have investigated the LVI positivity rate and its clinical significance in pT1b esophageal squamous cell carcinoma (ESCC) using immunohistochemistry and elastin staining.
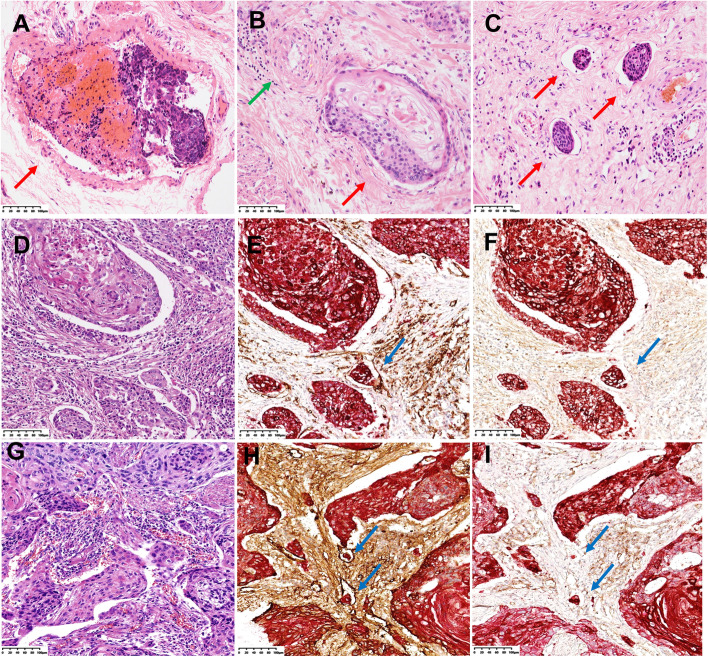
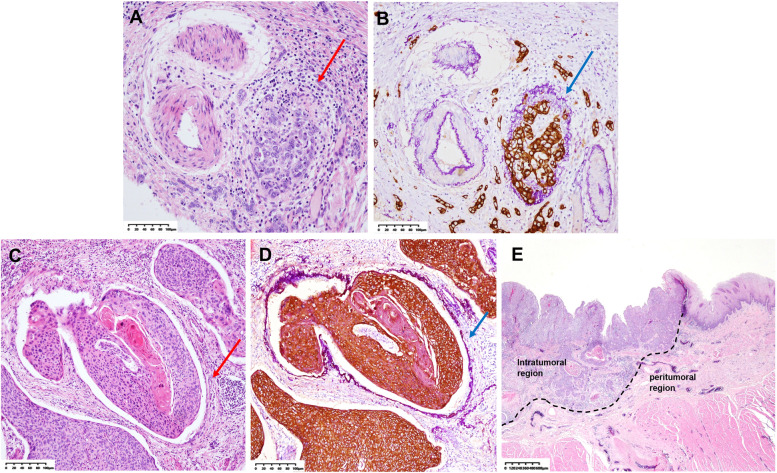
Methods: We collected data from158 patients with pT1b ESCC who had undergone radical esophagectomy. All paraffin blocks of invasive carcinoma from each patient were subjected to HE staining, elastin staining + CK (AE1/AE3) immunohistochemistry (E&IHC), and CD31/D2-40 + CK (AE1/AE3) double immunohistochemistry (D-IHC). The LVI was classified into types, i.e., vascular invasion (VI) and lymphatic vessel invasion (LI), and its location, quantity, and clinical significance were explored.
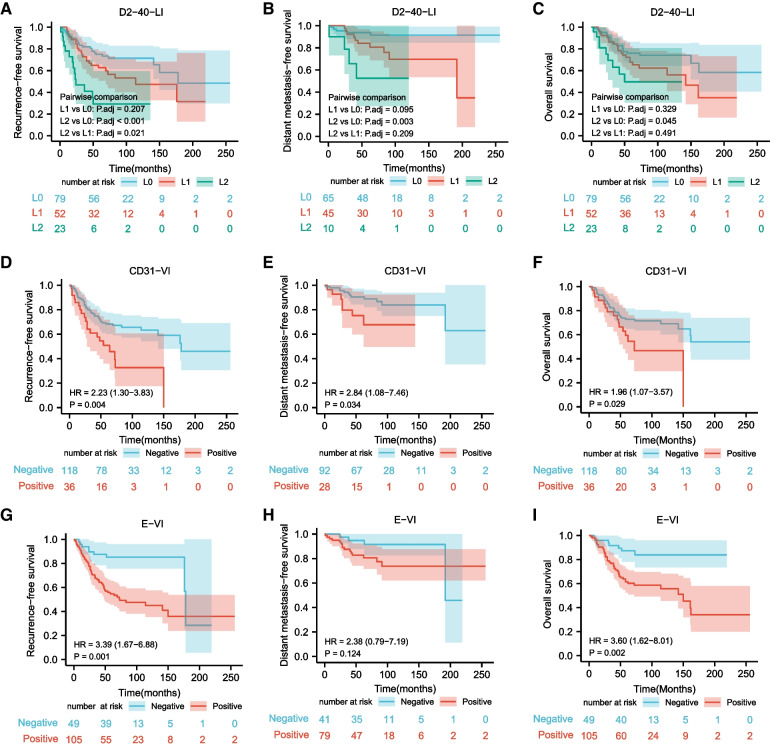
Results: The positivity rates of VI by E&IHC (E-VI), VI by CD31D-IHC (CD31-VI), and LI by D2-40 D-IHC (D2-40-LI) were significantly higher than those obtained by HE staining (P < 0.001, respectively). CD31-VI and E-VI were independent adverse prognostic factors for recurrence-free survival (RFS), and they were significantly associated with poor distant metastasis-free survival and overall survival in pT1b ESCC. Intratumoral LVI was also crucial in pT1b ESCC, and L2 (the count of D2-40-LI was 5 or more) was the strongest predictor for LNM and RFS in pT1b ESCC.
Conclusion: E&IHC and D-IHC can dramatically improve the detection rate of LVI in pT1b ESCC, and the classification and grading of LVI can help to improve the prediction of LNM and prognosis.
Keywords: Distant metastasis-free survival; Esophageal squamous cell carcinoma; Lymph node metastasis; Lymphovascular invasion; Overall survival; Recurrence-free survival.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO Classification of tumors Editorial Board . Digestive system tumours, WHO classification of tumours series. 5. Lyon (France): International Agency for Research of Cancer; 2019.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
