

Comparison of the application of high-flow nasal oxygen with two different oxygen concentrations in infant and child laryngotracheal surgery
- PMID: 37089587
- PMCID: PMC10113539
- DOI: 10.3389/fmed.2023.1169345
Comparison of the application of high-flow nasal oxygen with two different oxygen concentrations in infant and child laryngotracheal surgery
Abstract
Background: This study aimed to compare the use of the STRIVE Hi technique with 70 and 100% oxygen concentrations in children with 1st or 2nd degree laryngeal obstruction undergoing suspension laryngoscopic surgery.
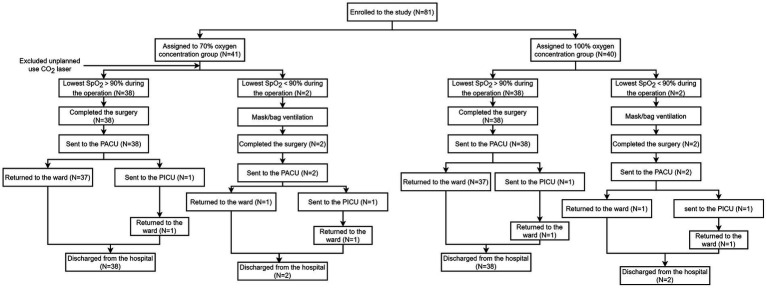
Methods: Children aged 1 month to 6 years scheduled for suspension laryngoscopic surgery with spontaneous respiration were randomly divided into the 70% oxygen concentration group (HFNO70% group) and the 100% oxygen concentration group (HFNO100% group). The data recorded for all the patients included age and sex, comorbidities, preoperative physiological status, methods of induction and maintenance of anesthesia, course of the disease and surgical options, and duration of operation. The primary endpoint was the lowest oxygen saturations during the surgery. The secondary endpoints included the partial pressure of oxygen PaO2, the arterial pressure of carbon dioxide PaCO2, the peak transcutaneous carbon dioxide PtcCO2, and the incidence of desaturation (defined as SpO2 < 90%) or hypercarbia (PtcCO2 > 65 mmHg).
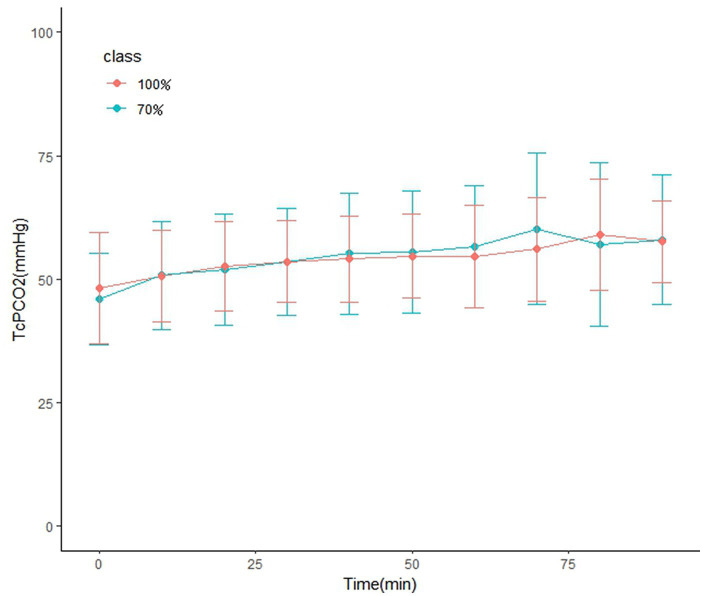
Results: A total of 80 children with 1st or 2nd degree laryngeal obstruction were included in the analysis. The median [IQR (range)] duration of spontaneous ventilation using STRIVE Hi was 52.5 [40-60 (30-170)]min and 62.5 [45-81 (20-200)]min in the HFNO 70% and HFNO 100% groups, respectively (p = 0.99); the lowest oxygen saturation recorded during the operation was 97.8 ± 2.1% and 96.8 ± 2.5%, respectively (p = 0.053); the mean PaO2 at the end of surgery was 184.6 ± 56.3 mmHg and 315.2 ± 101.3 mmHg, respectively (p < 0.001); and the peak transcutaneous CO2 was 58.0 ± 13.0 mmHg and 60.4 ± 10.9 mmHg, respectively (p = 0.373), despite a long operation time.
Conclusion: STRIVE Hi had a positive effect on children undergoing tubeless laryngeal surgery with spontaneous ventilation, and for children with 1st or 2nd degree laryngeal obstruction, there was no significant difference in maintaining the intraoperative oxygenation between the 70 and 100% oxygen concentration groups. The 100% oxygen concentration group showed significant hyperoxia, which has been proven to be associated with multiple organ damage. Using a relatively lower oxygen concentration of 70% can effectively reduce the hazards associated with hyperoxia compared to 100% oxygen concentration.
Clinical trial registration: [www.chictr.org.cn], identifier [CHICTR2200064500].
Keywords: STRIVE Hi; high-flow nasal oxygenation; hyperoxia; oxygenation; suspension laryngoscopic surgery.
Copyright © 2023 Liu, Xiong, Li, Du, Ru and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Thaung MK, Balakrishnan A. A modified technique of tubeless anaesthesia for microlaryngoscopy and bronchoscopy in young children with stridor. Paediatr Anaesth. (1998) 8:201–4. - PubMed
-
- Booth AWG, Vidhani K, Lee PK, Thomsett CM. SponTaneous respiration using IntraVEnous anaesthesia and hi-flow nasal oxygen (STRIVE hi) maintains oxygenation and airway patency during management of the obstructed airway: an observational study. Br J Anaesth. (2017) 118:444–1. doi: 10.1093/bja/aew468, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources