

Simulation-based Mastery Learning Improves Critical Care Skills of Advanced Practice Providers
- PMID: 37089675
- PMCID: PMC10117416
- DOI: 10.34197/ats-scholar.2022-0065OC
Simulation-based Mastery Learning Improves Critical Care Skills of Advanced Practice Providers
Abstract
Background: Advanced practice providers (APPs) are essential members of intensive care unit (ICU) interprofessional teams and are expected to be competent in performing procedures. There are no published criteria for establishing when APPs can independently perform procedures. Simulation-based mastery learning (SBML) is an effective strategy for improving critical care skills but has not been applied to practicing ICU APPs.
Objective: The purpose of this study was to evaluate if an SBML curriculum could improve the critical care skills and procedural self-confidence of ICU APPs.
Methods: We performed a pretest-posttest study of central venous catheter (CVC) insertion, thoracentesis, and mechanical ventilation (MV) management skills among ICU APPs who participated in an SBML course at an academic hospital. For each skill, APPs underwent baseline skills assessments (pretests) on a simulator using previously published checklists, followed by didactic sessions and deliberate practice with individualized feedback. Within 2 weeks, participants were required to meet or exceed previously established minimum passing standards (MPS) on simulated skills assessments (posttests) using the same checklists. Further deliberate practice was provided for those unable to meet the MPS until they retested and met this standard. We compared pretest to posttest skills checklist scores and procedural confidence.
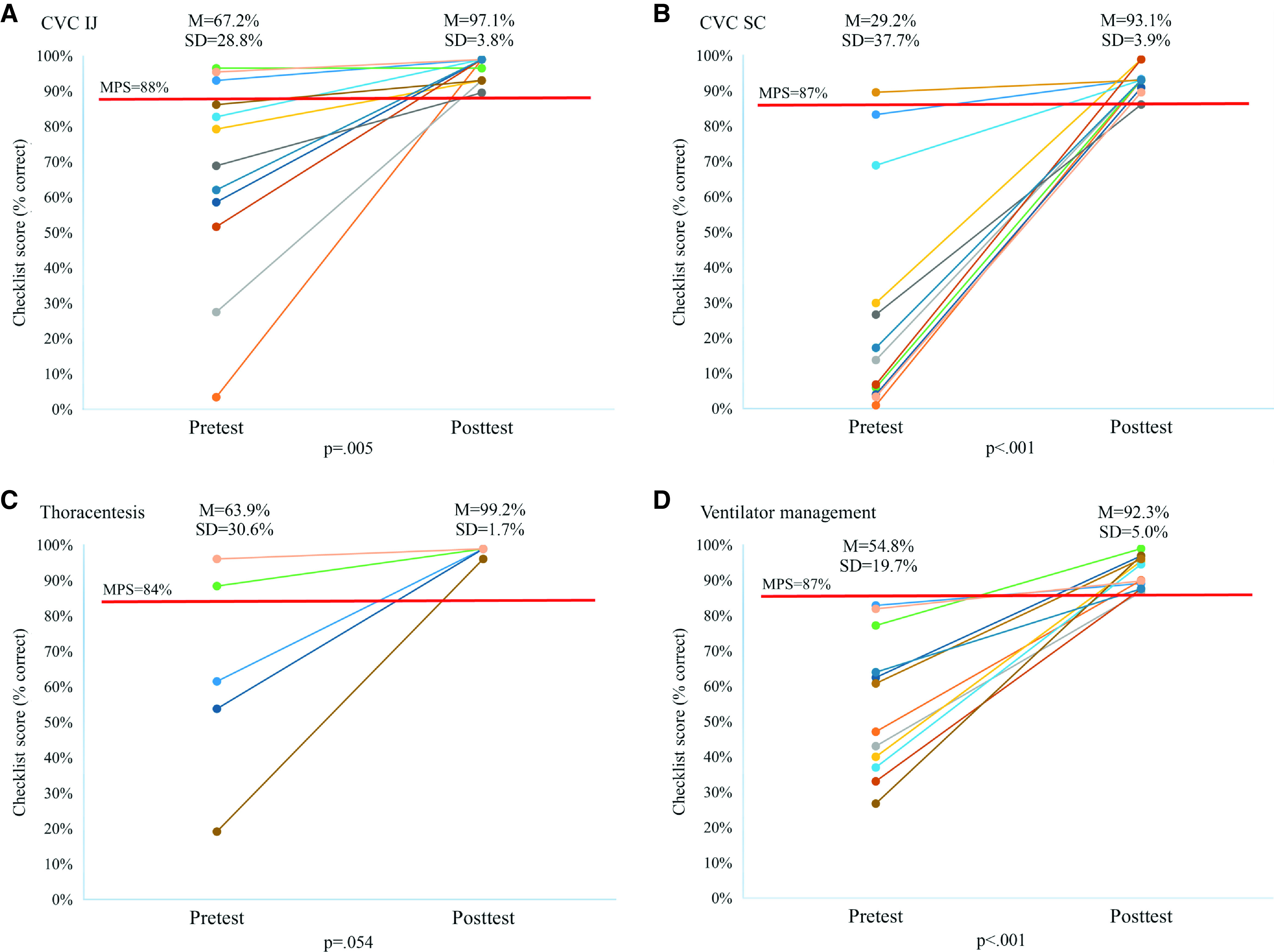
Results: All 12 eligible ICU APPs participated in internal jugular CVC, subclavian CVC, and MV training. Five APPs participated in thoracentesis training. At baseline, no APPs met the MPS on all skills. At training completion, all APPs achieved the mastery standard. Internal jugular CVC pretest performance improved from a mean of 67.2% (standard deviation [SD], 28.8%) items correct to 97.1% (SD, 3.8%) at posttest (P = 0.005). Subclavian CVC pretest performance improved from 29.2% (SD, 32.7%) items correct to 93.1% (SD 3.9%) at posttest (P < 0.001). Thoracentesis pretest skill improved from 63.9% (SD, 30.6%) items correct to 99.2% (SD, 1.7%) at posttest (P = 0.054). Pretest MV skills improved from 54.8% (SD, 19.7%) items correct to 92.3% (SD, 5.0%) at posttest (P < 0.001). APP procedural confidence improved for each skill from pre to posttest.
Conclusion: SBML is effective for training APPs to perform ICU skills. Relying on traditional educational methods does not reliably ensure that APPs are adequately prepared to perform skills such as CVC insertion, thoracentesis, and MV management.
Keywords: assessment; critical care; interprofessional; medical education; procedural skills.
Copyright © 2023 by the American Thoracic Society.
Figures
Comment in
- doi: 10.34197/ats-scholar.2023-0002ED
Similar articles
-
Impact of Simulation-based Mastery Learning on Resident Skill Managing Mechanical Ventilators.ATS Sch. 2020 Dec 23;2(1):34-48. doi: 10.34197/ats-scholar.2020-0023OC. ATS Sch. 2020. PMID: 33870322 Free PMC article.
-
Simulation-based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit.Crit Care Med. 2009 Oct;37(10):2697-701. Crit Care Med. 2009. PMID: 19885989
-
Use of a simulation-based mastery learning curriculum for neurology residents to improve the identification and management of status epilepticus.Epilepsy Behav. 2020 Oct;111:107247. doi: 10.1016/j.yebeh.2020.107247. Epub 2020 Jun 27. Epilepsy Behav. 2020. PMID: 32603805
-
Simulation-based mastery learning in gastrointestinal endoscopy training.World J Gastrointest Endosc. 2022 Sep 16;14(9):512-523. doi: 10.4253/wjge.v14.i9.512. World J Gastrointest Endosc. 2022. PMID: 36186944 Free PMC article. Review.
-
Beyond the simulation laboratory: a realist synthesis review of clinical outcomes of simulation-based mastery learning.Acad Med. 2015 Nov;90(11):1553-60. doi: 10.1097/ACM.0000000000000938. Acad Med. 2015. PMID: 26375271 Review.
Cited by
-
Mastery Learning to Prepare Advanced Practice Providers for ICU Procedures.ATS Sch. 2023 Mar 30;4(1):4-7. doi: 10.34197/ats-scholar.2023-0002ED. eCollection 2023 Mar. ATS Sch. 2023. PMID: 37089688 Free PMC article. No abstract available.
-
Impact of Simulation-based Mastery Learning on Management of Massive Hemoptysis.ATS Sch. 2024 Mar 15;5(2):322-331. doi: 10.34197/ats-scholar.2023-0120IN. eCollection 2024 Jun 1. ATS Sch. 2024. PMID: 39055331 Free PMC article.
-
Early introduction of simulation in the medical curriculum: the MedInTo perspective.Front Med (Lausanne). 2024 Jan 4;10:1280592. doi: 10.3389/fmed.2023.1280592. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38239607 Free PMC article.
-
Pediatric Critical Care Fellow Perception of Learning through Virtual Reality Bronchoscopy.ATS Sch. 2024 Jan 30;5(1):174-183. doi: 10.34197/ats-scholar.2023-0097IN. eCollection 2024 Mar. ATS Sch. 2024. PMID: 38585579 Free PMC article.
-
Effect of Polypectomy Simulation-Based Mastery Learning on Skill Retention Among Practicing Endoscopists.Acad Med. 2024 Mar 1;99(3):317-324. doi: 10.1097/ACM.0000000000005538. Epub 2023 Nov 7. Acad Med. 2024. PMID: 37934830 Free PMC article. Clinical Trial.
References
-
- Christmas AB, Reynolds J, Hodges S, Franklin GA, Miller FB, Richardson JD, et al. Physician extenders impact trauma systems. J Trauma . 2005;58:917–920. - PubMed
-
- Gillard JN, Szoke A, Hoff WS, Wainwright GA, Stehly CD, Toedter LJ. Utilization of PAs and NPs at a level I trauma center: effects on outcomes. JAAPA . 2011;24:34, 40–43. - PubMed
-
- Collins N, Miller R, Kapu A, Martin R, Morton M, Forrester M, et al. Outcomes of adding acute care nurse practitioners to a level I trauma service with the goal of decreased length of stay and improved physician and nursing satisfaction. J Trauma Acute Care Surg . 2014;76:353–357. - PubMed
-
- Kapu AN, Kleinpell R, Pilon B. Quality and financial impact of adding nurse practitioners to inpatient care teams. J Nurs Adm . 2014;44:87–96. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
