

A Genetic Risk Score Distinguishes Different Types of Autoantibody-Mediated Membranous Nephropathy
- PMID: 37090184
- PMCID: PMC10116192
- DOI: 10.1159/000529959
A Genetic Risk Score Distinguishes Different Types of Autoantibody-Mediated Membranous Nephropathy
Abstract
Introduction: Membranous nephropathy (MN) is the leading cause of nephrotic syndrome in adults and is characterized by detectable autoantibodies against glomerular antigens, most commonly phospholipase A2 receptor 1 (PLA2R1) and thrombospondin type-1 domain containing 7A (THSD7A). In Europeans, genetic variation in at least five loci, PLA2R1, HLA-DRB1, HLA-DQA1, IRF4, and NFKB1, affects the risk of disease. Here, we investigated the genetic risk differences between different autoantibody states.
Methods: 1,409 MN individuals were genotyped genome-wide with a dense SNV array. The genetic risk score (GRS) was calculated utilizing the previously identified European MN loci, and results were compared with 4,929 healthy controls and 422 individuals with steroid-sensitive nephrotic syndrome.
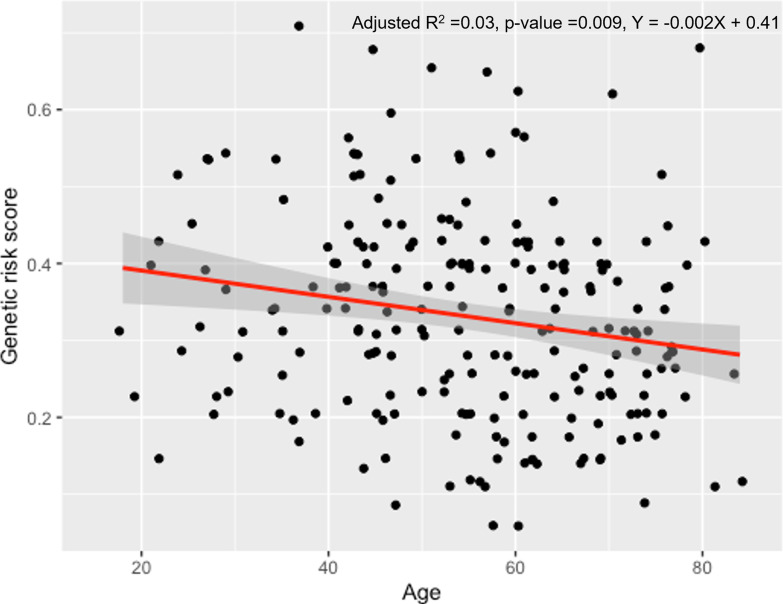
Results: GRS was calculated in the 759 MN individuals in whom antibody status was known. The GRS for MN was elevated in the anti-PLA2R1 antibody-positive (N = 372) compared with both the unaffected control (N = 4,929) and anti-THSD7A-positive (N = 31) groups (p < 0.0001 for both comparisons), suggesting that this GRS reflects anti-PLA2R1 MN. Among PLA2R1-positive patients, GRS was inversely correlated with age of disease onset (p = 0.009). Further, the GRS in the dual antibody-negative group (N = 355) was intermediate between controls and the PLA2R1-positive group (p < 0.0001).
Conclusion: We demonstrate that the genetic risk factors for PLA2R1- and THSD7A-antibody-associated MN are different. A higher GRS is associated with younger age of onset of disease. Further, a proportion of antibody-negative MN cases have an elevated GRS similar to PLA2R1-positive disease. This suggests that in some individuals with negative serology the disease is driven by autoimmunity against PLA2R1.
Keywords: Autoantibody; Genetic risk score; Membranous nephropathy; Phospholipase A2 receptor 1; Thrombospondin type-1 domain containing 7A.
© 2023 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- Pierides AM, Malasit P, Morley AR, Willkinson R, Uldall PR, Kerr DN. Idiopathic membranous nephropathy. Q J Med. 1977;46(182):163–77. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous