

This is a preprint.
A Comprehensive and Bias-Free Machine Learning Approach for Risk Prediction of Preeclampsia with Severe Features in a Nulliparous Study Cohort
- PMID: 37090627
- PMCID: PMC10120773
- DOI: 10.21203/rs.3.rs-2635419/v1
A Comprehensive and Bias-Free Machine Learning Approach for Risk Prediction of Preeclampsia with Severe Features in a Nulliparous Study Cohort
Update in
-
A comprehensive and bias-free machine learning approach for risk prediction of preeclampsia with severe features in a nulliparous study cohort.BMC Pregnancy Childbirth. 2024 Dec 24;24(1):853. doi: 10.1186/s12884-024-06988-w. BMC Pregnancy Childbirth. 2024. PMID: 39716098 Free PMC article.
Abstract
Objective: Preeclampsia is one of the leading causes of maternal morbidity, with consequences during and after pregnancy. Because of its diverse clinical presentation, preeclampsia is an adverse pregnancy outcome that is uniquely challenging to predict and manage. In this paper, we developed machine learning models that predict the onset of preeclampsia with severe features or eclampsia at discrete time points in a nulliparous pregnant study cohort.
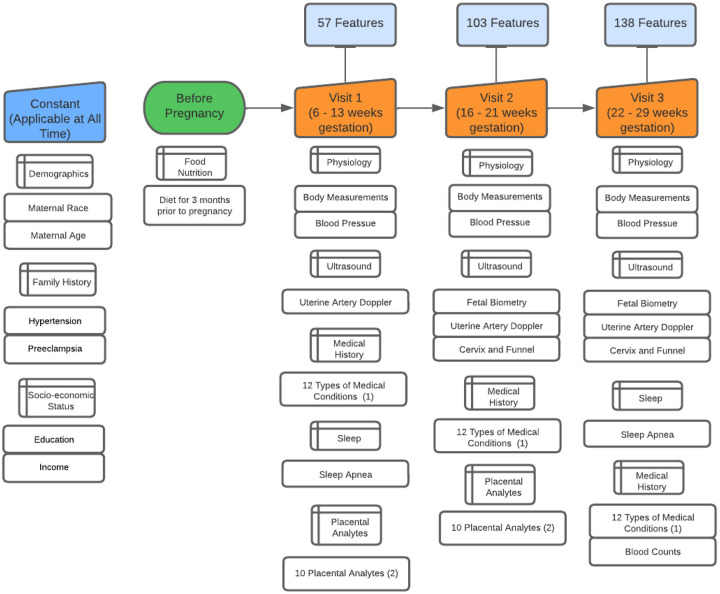
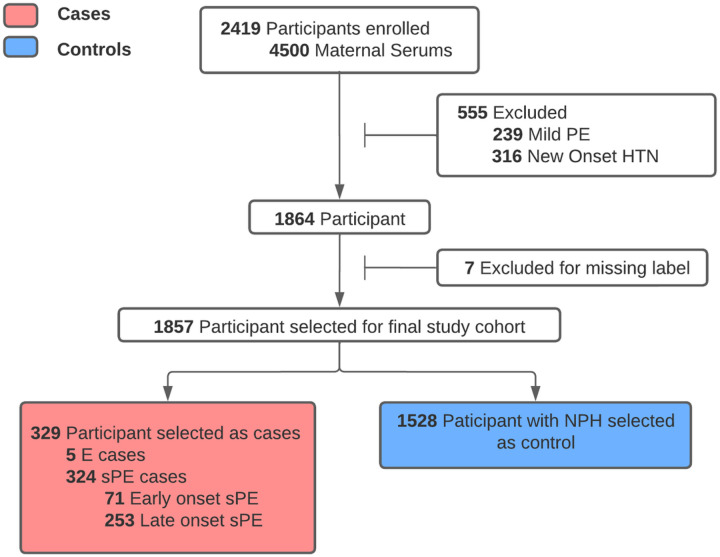
Materials and methods: The prospective study cohort to which we applied machine learning is the Nulliparous Pregnancy Outcomes Study: Monitoring Mothers-to-be (nuMoM2b) study, which contains information from eight clinical sites across the US. Maternal serum samples were collected for 1,857 individuals between the first and second trimesters. These patients with serum samples collected are selected as the final cohort.
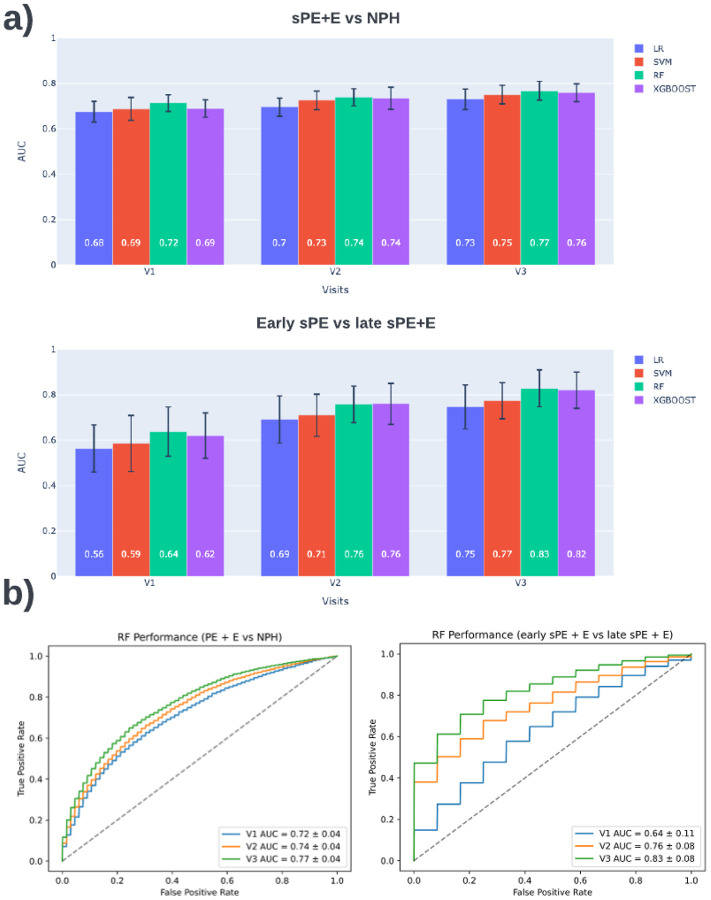
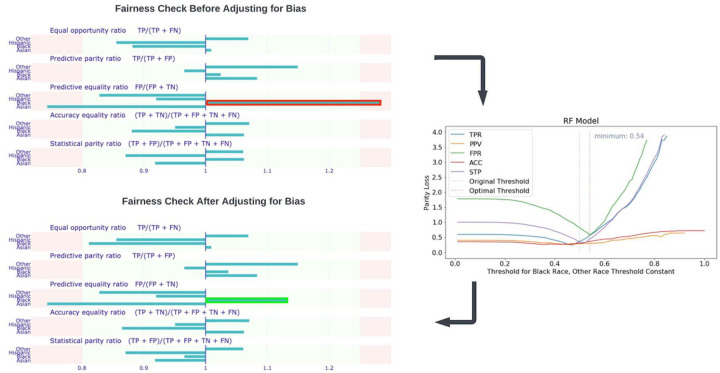
Results: Our prediction models achieved an AUROC of 0.72 (95% CI, 0.69-0.76), 0.75 (95% CI, 0.71-0.79), and 0.77 (95% CI, 0.74-0.80), respectively, for the three visits. Our initial models were biased toward non-Hispanic black participants with a high predictive equality ratio of 1.31. We corrected this bias and reduced this ratio to 1.14. The top features stress the importance of using several tests, particularly for biomarkers and ultrasound measurements. Placental analytes were strong predictors for screening for the early onset of preeclampsia with severe features in the first two trimesters.
Conclusion: Experiments suggest that it is possible to create racial bias-free early screening models to predict the patients at risk of developing preeclampsia with severe features or eclampsia nulliparous pregnant study cohort.
Conflict of interest statement
CONFLICTS OF INTEREST All authors declare no financial or non-financial competing interests.
Figures
Similar articles
-
A comprehensive and bias-free machine learning approach for risk prediction of preeclampsia with severe features in a nulliparous study cohort.BMC Pregnancy Childbirth. 2024 Dec 24;24(1):853. doi: 10.1186/s12884-024-06988-w. BMC Pregnancy Childbirth. 2024. PMID: 39716098 Free PMC article.
-
Placental protein levels in maternal serum are associated with adverse pregnancy outcomes in nulliparous patients.Am J Obstet Gynecol. 2022 Sep;227(3):497.e1-497.e13. doi: 10.1016/j.ajog.2022.03.064. Epub 2022 Apr 26. Am J Obstet Gynecol. 2022. PMID: 35487327 Free PMC article.
-
Using machine learning to predict the risk of developing hypertensive disorders of pregnancy using a contemporary nulliparous cohort.AJOG Glob Rep. 2024 Aug 22;4(4):100386. doi: 10.1016/j.xagr.2024.100386. eCollection 2024 Nov. AJOG Glob Rep. 2024. PMID: 39385801 Free PMC article.
-
Machine learning models for predicting preeclampsia: a systematic review.BMC Pregnancy Childbirth. 2024 Jan 2;24(1):6. doi: 10.1186/s12884-023-06220-1. BMC Pregnancy Childbirth. 2024. PMID: 38166801 Free PMC article.
-
First trimester preeclampsia screening and prediction.Am J Obstet Gynecol. 2022 Feb;226(2S):S1071-S1097.e2. doi: 10.1016/j.ajog.2020.07.020. Epub 2020 Jul 16. Am J Obstet Gynecol. 2022. PMID: 32682859 Review.
References
-
- Lockwood CJ, Moore T, Copel J, Silver RM, Resnik R. Creasy and Resnik’s Maternal-Fetal Medicine: Principles and Practice. 9th ed. (Dugoff L, Louis J, eds.). Elsevier - Health Sciences Division; 2022.
-
- Wójtowicz A, Zembala-Szczerba M, Babczyk D, Kołodziejczyk-Pietruszka M, Lewaczyńska O, Huras H. Early- and Late-Onset Preeclampsia: A Comprehensive Cohort Study of Laboratory and Clinical Findings according to the New ISHHP Criteria. International Journal of Hypertension. 2019;2019:1–9. - PMC - PubMed
-
- Sroka D, Verlohren S. Short Term Prediction of Preeclampsia, 2021.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
