

Parkinsonian Hand or Clinician's Eye? Finger Tap Bradykinesia Interrater Reliability for 21 Movement Disorder Experts
- PMID: 37092233
- PMCID: PMC10357208
- DOI: 10.3233/JPD-223256
Parkinsonian Hand or Clinician's Eye? Finger Tap Bradykinesia Interrater Reliability for 21 Movement Disorder Experts
Erratum in
-
Corrigendum to "Parkinsonian Hand or Clinician's Eye? Finger Tap Bradykinesia Interrater Reliability for 21 Movement Disorder Experts".J Parkinsons Dis. 2025 May;15(3):672. doi: 10.1177/1877718X251329129. Epub 2025 Mar 21. J Parkinsons Dis. 2025. PMID: 40114547 No abstract available.
Abstract
Background: Bradykinesia is considered the fundamental motor feature of Parkinson's disease (PD). It is central to diagnosis, monitoring, and research outcomes. However, as a clinical sign determined purely by visual judgement, the reliability of humans to detect and measure bradykinesia remains unclear.
Objective: To establish interrater reliability for expert neurologists assessing bradykinesia during the finger tapping test, without cues from additional examination or history.
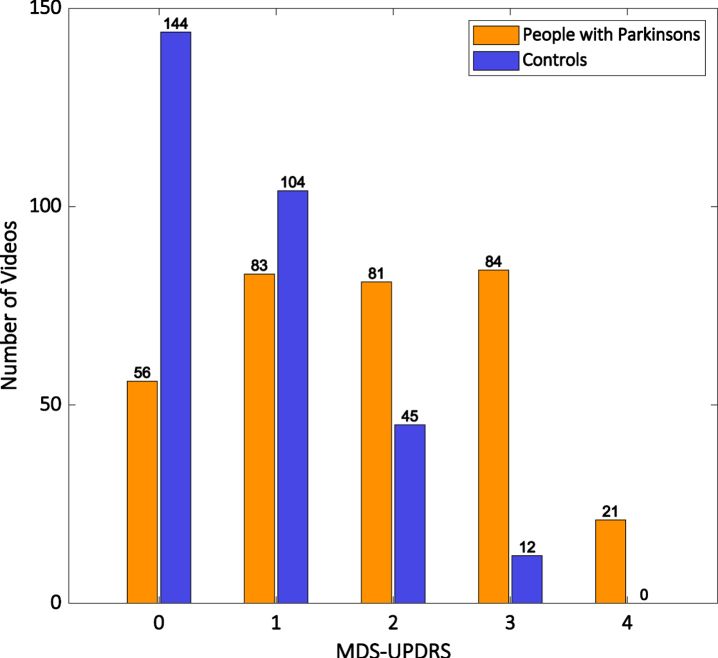
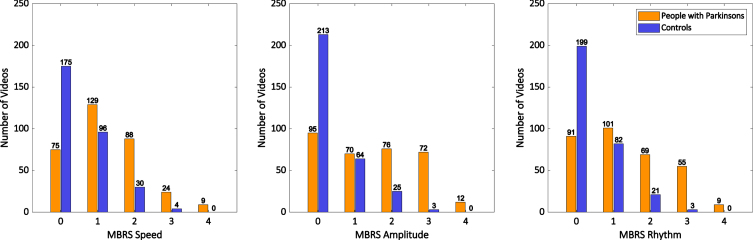
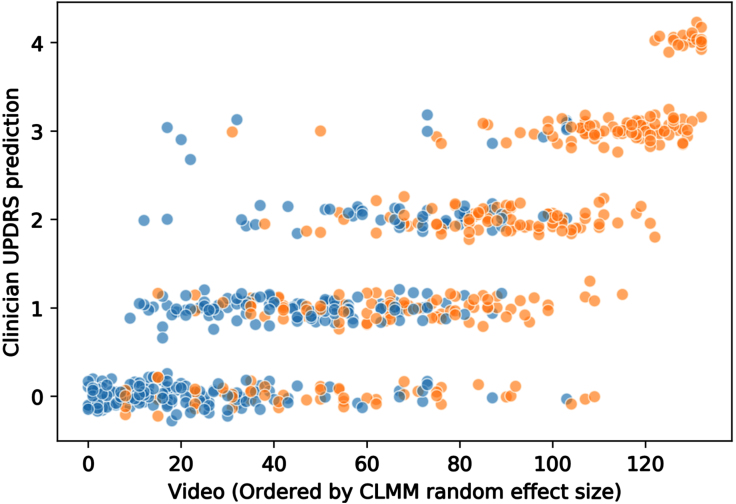
Methods: 21 movement disorder neurologists rated finger tapping bradykinesia, by Unified Parkinson's Disease Rating Scale (MDS-UPDRS) and Modified Bradykinesia Rating Scale (MBRS), in 133 videos of hands: 73 from 39 people with idiopathic PD, 60 from 30 healthy controls. Each neurologist rated 30 randomly-selected videos. 19 neurologists were also asked to judge whether the hand was PD or control. We calculated intraclass correlation coefficients (ICC) for absolute agreement and consistency of MDS-UPDRS ratings, using standard linear and cumulative linked mixed models.
Results: There was only moderate agreement for finger tapping MDS-UPDRS between neurologists, ICC 0.53 (standard linear model) and 0.65 (cumulative linked mixed model). Among control videos, 53% were rated > 0 by MDS-UPDRS, and 24% were rated as bradykinesia by MBRS subscore combination. Neurologists correctly identified PD/control status in 70% of videos, without strictly following bradykinesia presence/absence.
Conclusion: Even experts show considerable disagreement about the level of bradykinesia on finger tapping, and frequently see bradykinesia in the hands of those without neurological disease. Bradykinesia is to some extent a phenomenon in the eye of the clinician rather than simply the hand of the person with PD.
Keywords: MBRS; MDS-UPDRS; Parkinson’s disease; bradykinesia; finger tapping; interrater reliability; intraclass correlation coefficients.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures
Similar articles
-
Improving reliability of movement assessment in Parkinson's disease using computer vision-based automated severity estimation.J Parkinsons Dis. 2025 Mar;15(2):349-360. doi: 10.1177/1877718X241312605. Epub 2025 Feb 13. J Parkinsons Dis. 2025. PMID: 39973505
-
The discerning eye of computer vision: Can it measure Parkinson's finger tap bradykinesia?J Neurol Sci. 2020 Sep 15;416:117003. doi: 10.1016/j.jns.2020.117003. Epub 2020 Jun 30. J Neurol Sci. 2020. PMID: 32645513
-
Screening for Parkinson's disease using "computer vision".PLoS One. 2025 Aug 12;20(8):e0330373. doi: 10.1371/journal.pone.0330373. eCollection 2025. PLoS One. 2025. PMID: 40794744 Free PMC article.
-
Cholinesterase inhibitors for dementia with Lewy bodies, Parkinson's disease dementia and cognitive impairment in Parkinson's disease.Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD006504. doi: 10.1002/14651858.CD006504.pub2. Cochrane Database Syst Rev. 2012. PMID: 22419314 Free PMC article.
-
Physical exercise for people with Parkinson's disease: a systematic review and network meta-analysis.Cochrane Database Syst Rev. 2024 Apr 8;4(4):CD013856. doi: 10.1002/14651858.CD013856.pub3. Cochrane Database Syst Rev. 2024. PMID: 38588457 Free PMC article.
Cited by
-
Inter-rater reliability of hand motor function assessment in Parkinson's disease: Impact of clinician training.Clin Park Relat Disord. 2024 Oct 28;11:100278. doi: 10.1016/j.prdoa.2024.100278. eCollection 2024. Clin Park Relat Disord. 2024. PMID: 39552791 Free PMC article.
-
Artificial intelligence analysis of videos to augment clinical assessment: an overview.Neural Regen Res. 2024 Apr;19(4):717-718. doi: 10.4103/1673-5374.382249. Neural Regen Res. 2024. PMID: 37843200 Free PMC article. No abstract available.
-
Impacts on study design when implementing digital measures in Parkinson's disease-modifying therapy trials.Front Digit Health. 2024 Oct 9;6:1430994. doi: 10.3389/fdgth.2024.1430994. eCollection 2024. Front Digit Health. 2024. PMID: 39445101 Free PMC article.
-
Objective assessment of the effects of opicapone in Parkinson's disease through kinematic analysis.Neurol Sci. 2024 May;45(5):2035-2046. doi: 10.1007/s10072-023-07233-6. Epub 2023 Dec 13. Neurol Sci. 2024. PMID: 38091213 Free PMC article.
-
Computer vision uncovers three fundamental dimensions of levodopa-responsive motor improvement in Parkinson's disease.NPJ Parkinsons Dis. 2025 May 28;11(1):140. doi: 10.1038/s41531-025-00999-w. NPJ Parkinsons Dis. 2025. PMID: 40436873 Free PMC article.
References
-
- Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G (2015) MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord 30, 1591–1601. - PubMed
-
- Goetz CG, Nyenhuis D, Poewe W, Stebbins GT, Tilley BC, Lees A, Dubois B, Stern MB, Martinez-Martin P, Lang AE, Shaftman SR, Kulisevsky J, Dodel R, Sampaio C, Rascol O, Fahn S, Schrag A, van Hilten JJ, Holloway R, LaPelle N, Leurgans S, Olanow CW, Teresi JA, Jankovic J, LeWitt PA (2008) Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov Disord 23, 2129–2170. - PubMed
-
- Fahn S, Elton R (1987) Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease, vol. 2., Fahn S, Marsden C, Calne D, Goldstein M, eds. NJ. Macmillan Health Care Information, Florham Park, pp. 153-164.
-
- Martinez-Martin P, Gil-Nagel A, Gracia LM, Balseiro Gomez J, Martinez-Sarries J, Bermejo F, Jimenez-Rojas MC, Maranon E, Grau Veciana JM, Roig Arnall C, Bruna O, Junque Plaja C, Gimenez-Roldan S, Burguera JA (1994) Unified Parkinson’s disease rating scale characteristics and structure. Mov Disord 9, 76–83. - PubMed
-
- Kishore A, Espay AJ, Marras C, Al-Khairalla T, Arenovich T, Asante A, Miyasaki J, Lang AE (2007) Unilateral versus bilateral tasks in early asymmetric Parkinson’s disease: Differential effects on bradykinesia. Mov Disord 22, 328–333. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
